Good morning. I'm Me Karama Krishnan, one of the local
plastic surgeons, and uh.
Professor van La doesn't need any introduction after the talk.
Uh, we are going into this next session.
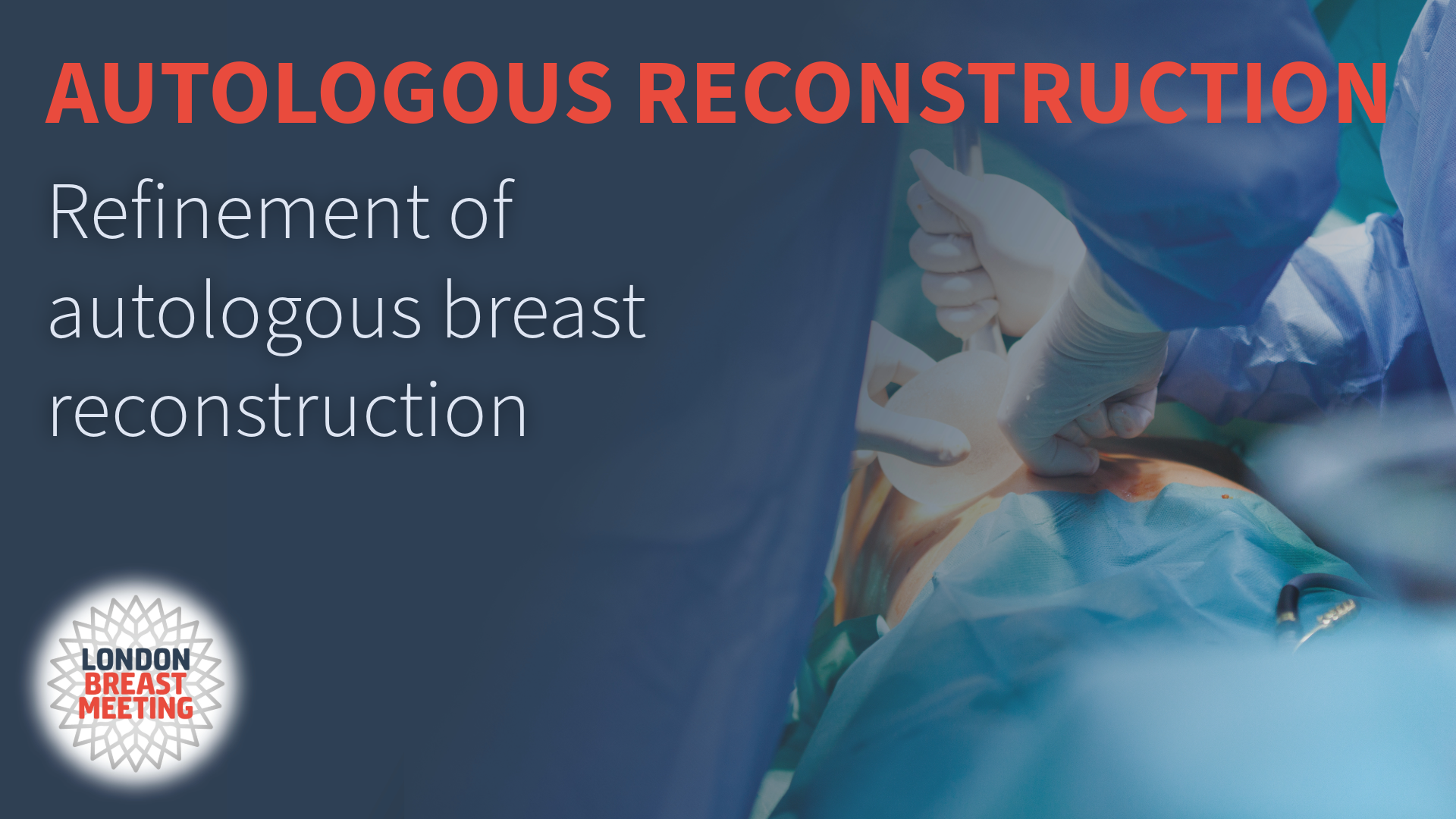
It's achieving gold standard in autologous reconstruction.
This whole session is going to be more technical.
The first speaker, I'll invite uh Professor Chang from MD Anderson to speak on nipple
sparing mastectomy, and free flaps reconstruction.
Professor Chang here.
He's just walking in. I
Very good. Uh, it's always an honour to be, uh,
a part of this meeting and thank you, uh, to Marlene Jian and Zhang Wei for including me.
Um, so this is sort of a deep dive into, um, doing a nipple spraying mastectomy
reconstruction. As a disclosure, obviously,
aside from being a speaker, but as a disclaimer, we do not do,
to be honest, that many nipple sparing mastectomies at our institution.
This again is sort of a collaborative effort with our breast surgeons and it's just a
philosophy at MD Anderson, that we don't typically do a lot of the nipple sparing,
um, the goal of this and the priority for our surgeons and the institution.
To cure and treat people for the cancer.
So oftentimes, you know, our breast surgeons, even for prophylactic cases,
will still explain to patients there's a risk for having recurrence of the nipple,
and we actually recommend removing the nipple complex.
So this again is a little bit of a difference in thinking in the paradigm compared to many
other institutions.
But again, obviously, you know, when you think about reconstruction,
nipple sparing versus Skin spraying mastectomies are vastly different from a
reconstructive perspective.
Obviously there's differences in an oncological perspective, but certainly for reconstruction
it makes a big difference. But again, taking a deeper dive into
reconstruction for a nipple sparing mastectomy, we have to consider certain factors that are
important in the details for the reconstruction. This includes the type of incisions from the
technical aspects and then obviously the management of complications.
So skin spar mastectomy is again a sort of the standard at our institution where The
mastectomy is performed through the nipple complex and again,
even with a skin spray mastectomy and autologous reconstruction,
we can achieve fairly reasonable results in patients even though we're sacrificing the nip
complex. However, when you think about the overwhelming
majority of studies published on this topic, the aesthetic outcomes,
patient reported outcomes, patient satisfaction is typically always higher when the nipple
complex is preserved.
So again for patients who Our candidates who are breast surgeons do deem candidates to
be undergoing a nipple scle mastectomy again, I think this does achieve very nice outcomes.
This is not with an autologous. This is obviously with an implant-based
reconstruction, but again for patients at our institution, the criteria is very,
very limited small breasted minimaltosis, good skin elasticity.
These are the candidates that our breast surgeons really select for and will offer.
nipple sparing mastectomy, and again I think we can achieve very reasonable results in these
specific circumstances.
But what about the details? What about the deeper dive into the nipple
mastectomy? Obviously the incision type makes a big,
big difference. When you look at all the studies that have been
published on this topic about the incision type, the overwhelming majority will all say
any type of incision that is peri areolar, whether it be a To hat,
a superior incision with a lateral extension, anything that is around the areola has a higher
risk for nipple necrosis and again that intuitively makes sense when you've done the
mastectomy and you've interrupted the blood supply coming in through the breast tissue,
if you make an additional incision around the nipple or complex,
you're further compromising the perfusion to the nipple complex and again your risk for uh
nipple necrosis is gonna be much higher.
So again, if we can. Ideally we want to do the nipple square
mastectomy through an inframammary incision. The inframammary incision again tends to be the
preferred incision of choice because the rates of nipple larial necrosis are fairly low
compared to a periareolar incision. And again for patients who are deemed
reasonable candidates for nipplesper mastectomy, our breast surgeons ultimately do make the
choice because from their perspective, even though the risk of nip complex necrosis is
lower, the tech. aspects of performing the mastectomy through
incision are much more difficult, so some of our breast surgeons will still opt to use a per
incision. So this again is going to be potentially at a
higher risk for compromise.
We were fortunate in this case again it's obviously a technical achievement by our breast
surgeons, but again, statistically speaking, based on the evidence,
the risk of necrosis is much higher when you use a periaal incision.
But how does this factor into autologous reconstruction?
If you're doing an IMF incision, your ability to reach a recipient vessels is a bit more
challenging because you're at a much lower level.
We typically use the third intercostal space, identify and use a recipient vessel's internal
mammories at the 3rd intercostal space.
If you're at the IMF, it can be potentially more difficult to reach your internal memory.
Vessels at the proper inner space.
If you have to go to a lower inner space, this is particularly relevant if you're dealing with
the left side, not so much as the artery, which is equivalent from the right to the left,
but the vein is significantly smaller on the left side.
So if you're at an inframammary incision.
At a lower inner space, you have to be aware that potentially you may be dealing with a
lower, smaller calibre and vein which again may potentially put you at risk for complications
during an autologous reconstruction. So again,
you have to be thinking about alternate recipient vessels or potentially lengthening
your incision or doing some manoeuvre in order to gain you access into a higher inner space.
How does this also factor into flat monitoring? So again,
when you're doing. brain mastectomy, you're sparing all of the
skin and the complex. So what do you do with your skin paddle?
By far and large clinical exam is regarded as the gold standard.
There are a lot of different technologies that are out there,
but none of these really supplant the use of clinical exam.
This includes evaluating the skin for temperature, colour,
urger, warmth, and obviously a Doppler signal.
But again, I would say, you know, if you're saving the skin.
Paddle here. This is obviously not a nipple sparing,
but this was a nipple sparing side.
She didn't want to go back for excision of that monitoring segment.
For me it's sort of embarrassing because then I have to show you these photos and you're like,
God, this clown's like doing the most horrible results and why is he speaking.
But this again just to illustrate that this again for me is not a very nice cosmetic result.
But again, clinical exam is going to be the gold standard for flat monitoring,
and this is just again a plug for our sponsors T set upstairs.
You can use. A lot of different techniques in order to
monitor your flat, but again, clinical exam is still the best.
This again a very suboptimal result, and our breasts opted to go with a top hatch incision.
Again, it's not a bad option to get to.
It helps us though because this incision is higher on the chest wall,
so your access to your recipient vessels, you can usually get into the proper inner space
versus going lower down. And again, after a revision you can excise the
skin paddle. The scars maybe not as great because you have
that, but again, sort of considerations when you're doing a nipple sparing mastectomy.
So nowadays, oftentimes for many of us at our institution, probably across the country,
a lot of people will use or incorporate the use of an implantable Doppler for monitoring.
This again, while fairly accurate, sensitive and specificsia are not nearly as good as a
clinical exam, so something again to be cautious of complications that can happen,
obviously this is a Young patientsaspogastric banding has some massive weight
loss and again as a candidate for and surprisingly for a nipple mastect by our breast
surgeons, but again this is sort of like the dreaded complication,
right, you know, partial necrosis of the nipple complex ultimately don't debride this if it's
not full thickness, let it heal by secondary attention and again we lost some pigment here.
Uh, we offered her to tattoo this but again she was sexually.
OK with it she's like this sort of my badge of honour sort of going through and she was
actually OK with it um but again this is a potential complication that you will have to
potentially manage during nipple spar mastectomies.
This again is another dreaded complication maposition.
We need Dr. Mallucci to come and show us how to medialize
this nipple error complex, right?
This position is horrible, so I'm gonna send this lady here to London for him to fix,
but this again becomes a very challenging.
issue to reposition the nip complex and this again was an interesting incision.
Our breast opted to go with a vertical incision, which again is not necessarily terrible if you
need to reduce the skin envelope. This again allows you to do that through that
incision. But what is the sort of the ideal
reconstruction, ideal candidate for patients undergoing nipple sparing mastectomy and
autologous reconstruction? We typically have always used the abdominal
donor site. A patient is not a candidate for the abdominal
donors or deep flap.
Now our next choice is the inner thighs the path or the profund artery perforator flap is
our next flap choice of option.
We're not nearly as talented as Coon, so I can't do a lumbar artery with any degree of
success, but again, this is sort of the ideal patient.
No breast cancer, atypical ductal hyperplasia, small breasts,
no ptosis, minimal ptosis.
And relatively thin young, good skin elasticity, and again we opted to reconstruct it with path
flaps. The pedicle for the path flap, the artery and
the vein, are typically smaller.
So through the IMF incision, if you can only access the 4th inner space,
this actually coincides very well and has a very nice skin or size match for the internal
memory vessels and your recipient vessels and again postoperatively scar very well concealed
in the infra memory fold and again. Able to give her a very nice results.
Here's a young patient who underwent nipple spray mastectomy and implant-based
reconstruction has rippling and doesn't like her implants and again wants to exchange them
out for autologous tissue.
And again her circumstance we have been doing stack PADla to give her the necessary volume
and again postoperatively doesn't have the volume and the projection necessarily of her
implant-based reconstruction.
We did leave the skin paddle for monitoring, which is actually pretty well concealed.
offered her to go back to exercise that she declined, but again,
I think for a patient with a good skin elasticity that has minimaltosis,
not looking to be very large, again, I think these patients are sort of the ideal patients
for nipple sparing mastectomy reconstruction.
So in conclusion, I think, you know, I think without question most people would agree that
preserving the nipple complex really gives patients the best overall cosmetic result when
you're thinking about doing autologous reconstruction.
Though there are a lot of considerations that you have to think about to try to minimise
complications, but part of the most important thing, single most important thing is get a
great breast surgeon.
The ability to preserve the nipple and do the mastectomy safely is really dependent and
working very collaboratively and collegially with the breast surgeons because that is really
going to be the most single most important thing in my opinion in order to achieve a nice
result. Thank you so much.
We have Doctor Andrea Moreira, talking about
aesthetic considerations, the patient versus surgeon outcome.
It's nice to come after you had because you talked about a bunch of stuff that I had to
talk, so it's good.
All right, so we published this study a few years ago and it's called The Beauty is in the
Eye of the Beholder. What we did, we actually compared and
correlated what the patients responded on the Quality of Life questionnaire using the breast
cue with photographs of the same patients at the same time point that they responded to
breast cue. And we asked observers, 30 party observers to
actually rate um those um those photographs and what we found with this study was actually
very interesting. In 33% of the cases, patients and observers
agree with the cosmetic outcome, but in about 36% of the patients there was a clear
disagreement. And what we found is that patients who had a
good response and a good quality of life on the breast scale perceived the reconstruction
better and the ones who had a poor quality of life perceived the reconstruction as worse.
And I just want to point out to that outlier over there.
This patient was rated by the observers as the best reconstruction.
And she graded her reconstruction as the worst, so there's clearly,
you know, a big difference.
And what we found out is that the psychological and social well-being and the physical
well-being played a role in this.
But we also found out it was a weak correlation that patients who had delayed reconstruction
were more satisfied than the ones who had immediate reconstruction.
Maybe the loss of the breast for some time played a role in that.
But just to show you a few examples, this patient was rated by the observers as a
fairly bad, um, reconstruction result, and I agree, but she was one of the most satisfied
patients, whereas this one who has a very good cosmetic outcome if you think about it,
um, hated the reconstruction.
So there's a lot that we need to understand when we discuss outcomes with our patients,
but the truth is that breast reconstruction nowadays, we moved from creating breast mounds
and making the flap survive to actually create an operation that is almost like a cosmetic
procedure. We're actually recreating breasts and now even
sensate breasts, right?
Um, I do like to point to the Angelina Jolie effect.
Um, I think this was great when it happened. It created a lot of awareness.
Patients are much more participative on their, on the discussion,
but also create a lot of anxiety.
These patients now, they look towards reconstruction and they want to have this
perfect body. Uh, sometimes it's achievable.
We saw that yesterday, but sometimes there's a lot of unrealistic expectations.
And I do point social media for that because I think social media has the good.
There's a lot of information.
There's also a lot of misinformation. There is plain dishonesty too,
and that really plays a role on how the patients uh behave towards their reconstruction.
So in my practise, I think successful reconstruction is really no details.
The initial consultation is extremely important. You have to be super through with the patient.
You have to show them what's real and what's possible.
Um, I do like to optimise my patients for surgery.
If you go to the American.
Of surgeon's website. There is a programme called Fit for Surgery.
It's actually excellent you can download and it really helps.
Um, in terms of the surgical procedure, you wanna make sure that you're safe.
You want to minimise complications, and you really have to pay attention to pain control.
Pain control is one area that the patients will rate their final result as for,
is that the pain is not well controlled. And of course,
postoperative education, be prepared for revision surgery.
So I do an ERAS protocol for all my patients. It's very standard.
It's pretty much what has been described.
The only thing that I added and has been a game changer is actually intrathecal morphine,
and it's done just before they go to sleep.
These patients complain of zero pain. For pap flaps,
it's absolutely wonderful.
So, um, I think it's one more thing that can be added to the pain control for these patients.
Um, I'm not gonna talk too much about nipposparing mastectomies with in our
institution is a rule, not an exception, and, uh, one thing about it,
you have to make sure that you are in very good relationship with your breast surgeon.
So, um, the boundaries of the breast are. Maintained and the skin blood supply is
maintained, but I really suggest that you reconstruct any violation of the IMF lateral
breast border, medial breast border before you actually insert your flap.
After that, it becomes really difficult.
Um, you know, I do my anastomosis on the 4th or 5th intercostal,
both because most of my patients get an IMF incision.
The vessels that are a little bit smaller, but access to the vessels is much easier and I hate
to struggle on the 3rd or 2nd intercosis.
in a situation like that and you please try to avoid traction injury because this happens.
So you have to do your ostomosis fast, can't retract that ski very much and going lower on
the rib, I think it helps.
Um, um, and, and of course, try to preserve the nerves, you know,
we know that if, if you get to the lateral back muscle, you're gonna start seeing all these
ecostal nerves going to the mastectomy skin, preserve them.
There's no need to divide them.
So, uh, but if you do that, in general, your patients will have a better recovery of
sensation and uh we actually published our technique, um,
on how to preserve these nerves.
Sometimes the nerves are divided and if that's. Situation where you can do it is actually a con
uh mentioned on the stock.
You can actually find uh sensory branches at the abdominal flap,
and you can dissect the intercostal nerves at the chest while they run perpendicular to your
vessels, and you can connect either a nerve graft or an autograft to your flap,
and over time, there's plenty of studies. Estefania Twinder is a champion on this.
It shows improvement of sensation over time.
Um, I do like to talk about the abdomen. I think this was overlooked in the past.
Uh, in my mind, you have to address the abdomen. There is nothing worse than you do this
gorgeous breast reconstruction and you you look at your patient's belly I'm like,
oh my God, why did I do this?
So, in my practise, you wanna avoid um wound issues and for me,
doing a limited lateral undermining is important.
I always placate my patient.
Um, you have to pay attention to the location of your umlycus,
and you wanna lower that abdominal scar as much as possible.
And talking about minimising trauma to the rectus, um,
this is an open deep on this side so you see how much disruption,
even if we reconnect the nerves, a lot of disruption to the abdominal wall,
um, if you attempt to do a robotic d and that was a.
Later robotic deep here you can actually minimise the trauma and the damage to that
abdominal wall and you have a more sort of uh satisfied patient just to show a case very
quick, this is a patient that you guys saw yesterday.
She had a direct implant um to the right side. She hated her implant,
so we went, uh, for a bilateral jeeps, um, again, limited undermining.
I marked the area to be placated. The placation is done.
I use VLo for that.
Um, now, the particle for the perforator flap is dissected through a limited
incision. We published this technique.
It's, you can take a look, and the rest of the dissection is done using the robot in an
intraabdominal approach.
That's her result after surgery, so low. The abdominal scar like Kate,
so you have a better incision line and pay attention where you place that belly button.
This is another case. She's a BRCA2 patient and bilateral
reconstruction with JP 3 flaps and the robotics and really good abdominal function six weeks
after surgery. Now, talking about the umlycos position,
I think it's an illusion.
In general, we place the umbilycos based on the iliac crest,
but if you do that many times, the incision for the GIP flap is higher than that and your
umlycos is gonna look very low.
So I, I pretty much use what Hoyos described. As well as Maia Sagareo,
um, I divide the abdomen in third, beginning from the xiphoid down to the incision,
not the Rafi, and I divide it in 3s and the umbiliccos go in the inferior third,
and I think over time you can get a really good position of the umbiliccos that way just to
show um. A few cases.
This is one of my patients, um, very good placement of the umbilicos that makes a big
difference for them. This is a patient that came to me for a
revision. In my mind, this is a completely unacceptable
result. You have a high scar, you have a lowlicos,
the flaps don't look right.
So for this patient, I actually did inserted her umbilicos.
I lowered her abdominal scar and I revised the breast is not perfect,
but at least it's better than what it was before.
Now, uh, we know that satisfaction with.
Uh, the breasts increase with revision procedures.
And for that, usually you can address the breast by taking the skin paddle,
uh, of the GIP free flap. You wanna reshape the flap.
Take advantage of fat grafting because it's really good.
Mastopexy reduction, liposuction, um, and for abdomen, I usually revise scars,
lower the incision if it's necessary, and, uh, liposuction.
I do a very extensive liposuction on my cases, um, and I,
I joke that I'm probably.
Paid for it, but the truth is taking this axillary fat pad,
you know, lipo the abdomen, giving them a better contour,
liping the mounds because sometimes it gets really full and lower the abdominal scar,
you can actually get a pretty good result.
Um, and your revision might be just a nipple reconstruction like this lady.
She didn't want anything else.
So, uh, I think it, it's a home run. She didn't want her nipple her breasts to be
higher. She was very happy.
Uh, in a case like that, she was radiated to the right side.
I did. The liposuction, lower her scar, um, and uh use
fat grafting is a great adjunct um nipos perioasstectomy, you know,
it's just so looks so natural that you can even tell that these patients had surgery and you
can even offer these procedures for patients who have unfavourable bodies,
um, like this lady who has BRCA positive, had a bilateral deeps.
So, um, the big message, um, that I wanna, uh, give to you is that for satisfaction.
Either patients or surgeons.
It goes really beyond the reconstruction. You have to understand your patients,
so you can actually offer them what's the right procedure.
Complications played a big role in it. If you have complications,
they will receive the. Reconstruction as worse,
um, you wanna get good outcomes, um, and we really should track our patients and look at
the breast cue because that's what's gonna give us a very good idea of if what we're doing is
the right thing for the patient.
Thank you so much.
Thank you. The next speaker is uh Gemma Ponds,
needs no introduction from Clinica Plan Us. She's going to talk to us about fat necrosis
and how to avoid it. Thank you very much,
Marlene and Jan for having me here.
It's like it, it's not my main topic, but I can say something about what necrosis.
So I'm going to talk about uh our strategies.
You know, this is the uh one of the cases that we often face and ah if you are too optimistic,
you end up with a fat necrosis ah in the patient and it's it at the middle
part of the breast that is really difficult to, to solve.
And ah ah this is even a worse case that if you just looking what's happening,
you don't act, you, you end up like this situation that you,
you, you, you can try to control with this device, but at the end,
ah, most of the cases, uh, you will end up with these situations that ah sometimes it's better
just to start from the beginning.
And if you remember what the uh JP said yesterday, we end up in these situations with,
when uh we just watch what is happening or we really don't know what is happening.
So, I in more than 20 years ago, we just knew very limited information about
perfor flaps and then when we got into trouble, that what we didn't know what exactly what was
happening, but nowadays we, we know, ah we, we know almost everything about the anatomy and
the physiopathology of the flap, and we have all the different tools and strategies ah to
just perform ah ah ah the, the safe reconstruction for the patient.
So for us to reduce the risk of a necrosis, we can act in different moments before
the surgery, during the surgery, and after it.
Before the surgery indications are key and also the preparative planning during the surgery,
the surgical technique counts and also the interparative assessment.
And then after the surgery the follow up just to to realise when the problems are starting
and to act as soon as possible.
About the strategist as Professor Marcia says many flaps just died before the surgery because
the planning has not been the correct one.
And surgical indications are also some some point that we have just to be aware.
We know that we have to be aware in obese patients, in the smokers when they are having
abdominal scars, liposuction, radiation.
They are not contraindications, but we have to know beforehand to uh just uh to control during
the surgery any uh any just bad situation.
And on the other hand, there is literature saying that when we are performing uh bilateral
reconstruction, especially in the flap, it's a protective factor.
This is just because we are just uh using less amount of tissue.
City angiography, uh, it's a, it's was just described for by our group many years ago
and uh as you know, it permits just a visualise beforehand what we are going to find out during
the surgery and it gives mainly anatomical details about the the the vessels.
It permits us to identify the dominant perforator of our tissue and we believe that
it's nowadays a standard properative imaging.
It permits us to, to really define the vessels to transport transfer that
information into the patient with really exact precision.
We can assess also the superficial system, we can assess uh the,
the, the, the vessels, the artery, the vein, the exit point where the vessel is piercing and
um also uh just to have the whole information uh into the tissue.
And uh do we really need this uh this information?
It's that in expert hands in expert by expert surgeons, they can uh have that extra
information uh before because of the experience and that uh they may not need
it, but uh really the CT angio permits that you have to have a more safer and predictive
surgery and at the end to reduce the risk of necrosis.
Also, in thermography can be used because it can just,
uh, you can obtain information about the hot areas that is the exact areas where the
perforator is piercing and to know exactly where that that vessels are and also after
raising the flap, what are the uh the better nourished uh uh tissue.
the introvertive strategies, we know that city and geography gives very anatomical information,
but it really lacks of physiological information.
And because of that we complement interpretively with ICG and geography because
it permits just tailor our flap and just discharge those black areas that they are
poorly perfused and with that you really can diminish the rate of fat necrosis
and especially because when you are too optimistic.
Especially in the peripheical areas that you want to preserve and then you add that
extra sutures to to at the time of the shaping you you you can have many high
chances to have fat necrosis in that very physical areas.
On the other hand, ICT and geography permit also have information.
About the perforreto is really uh entering the the the the the vas into the flap and as
you can see in this video of a lap flap, you can see that all the whole uh flap just
with one refrigerator is completely profuse and you can just compare with the demographic
information. So with the property uh planning with CT and
geography, we can have anatomical information and with the ICT angiography we can have the
physiologic ormodynamical information.
And with that we take advantage of all the technological progress and we can offer our
patients very safe information. And this is especially important in more
complex flaps like scab, lumbar, SIA when you only have one vessel and if you get into
trouble, you really can, you can lose the flap.
But in the flap, we have all the the different uh uh uh the choice of
of of vessels and we know nowadays how we combine them in order to just offer a
safe surgery.
We know that in a flap like that with a huge vessel that is centred in the middle of the
flap, it's very difficult to have uh to get into trouble.
But nevertheless, as a standard approach we always dissect a a small length of our
superficial epigastic vein.
Uh, uh, because, uh, it really can, uh, just save, uh,
many flaps like in this case that you can see that uh it needs that extra vein that we just
to most, most of the cases to, uh, any vein in the axilla.
Also, uh, if you suspect that you can get into trouble, the profeor are very small or they are
very veryerical or you are just willing to use the whole flap.
Uh, you, uh, in cases like this case, you have two perforators in the same row,
you can dissect both of them.
And just very occasionally if you can find 3 perforators like in this case in the same row
without the need to uh to to just cut the muscle, you can dissect all of them.
Uh, also, uh, in, in this case, you have a very peripheical big perforator,
but if you need the whole flap, you can just perform in the flap and ostomosis,
uh, between two perforators to just perform a safer raising of the flap.
And also this was a case and we needed the whole lap and we wanted to use the perforators
but we also we wanted to preserve the muscle, so we just dissected both of them then uh we uh
below the muscle we cut one of the perforators and then we performed perforated perforator and
we could just preserve the whole uh uh abdominal anatomy.
And most importantly, the technique is in cases like that when you have to perform a very huge
uh resection uh with the breast and and part of the ribs and if you fail in,
in some small part of the flap, you can just get into uh big troubles in this patient.
This patient had just limited toor side, she's very young,
so we just decided to perform.
reconstruction with the LDT uh razor flap that was the resection including the ribs
and that was the reconstruction that uh that the thorastic surgeon performed and this is
just the, the razor flap, the tap and then LD and just with one on our side we just put
uh solve the, the, the reconstruction of the chest.
And just to finish the postoperative strategies, we know that clinical is the key.
Uh you just have to go to check to train the residents to train the,
the, the, the nurses, but also we use in our hospital the near infrared spectroscopy
that is uh that the the anesthesiologist and also neurosurgeons use,
and this is very useful because if you have lazy residents.
And they don't want to wake up at night, uh, that just give information before the clinical
signs, uh, arise.
It just gives information about uh the exigination of the flap.
So then it's when the nurse can call the, the resident and And that is the the way that you
can act early.
So just to finish, if you want to become like a GP, if you want to make uh just uh things
happen, just act as early as, as possible and remember that uh the
uh before the surgery is. The Planning is key.
Use all the technology, all your knowledge that you have,
the technique, and also if you have available ICG you can offer safer surgery and of course
uh the follow up is the final point and as important as the,
the, the previous one.
And uh just to finish, remember that uh next year in Barcelona,
everything is happening in on March the we have the Barcelona meeting and on April WM and
we just are waiting for all of you. Thank you very much.
Discussion. We'll have some uh discussion now uh are there
any questions on the floor?
Thank you. uh, I have a question for Doctor Moreira.
I really enjoyed your talk and I think you pointed out very key.
Uh, um, things about breast reconstruction and I am especially curious about the restoration
of sensibility.
How do you do it and most importantly, how can we evaluate in the post op to see what we're
doing is actually working for our patients. Thank you.
Yeah, so, um, I'm gonna answer the last question first.
So what we do in terms of monitoring, we, we get a pre-op baseline for the patient.
Uh, we know it's gonna be normal sensation, but many times it's not normal sensation.
I think it's really important, and we do two point we don't do two-point discrimination
because it doesn't work that well.
We do Samwman, um, and there is a study going, uh, forward,
but we don't have the full answers about using vibration also.
And in terms of postoperatively, I usually test my patients a month after surgery because
in my mind, whatever is there at a month is preserved sensation.
Then I test at 3 months, which is also preserved sensation.
It's nothing that I, there's no nerve that I connect that it's gonna grow that fast,
but usually we see recovery sensation after the nerve graft begins to work.
It's usually after 89 months.
So you need a longer follow-up and uh you really need about 2 years to follow up these
patients. And the key is to do the testing.
Um there is for the new breast cue, a whole session on sensation.
Um, I think it's good to correlate that to what the patient is feeling,
right? But in terms of the technique, um.
Our paper describes very well on how you can preserve some of these nerves,
but the key is when you get to the lateral chest wall dissection,
the moment that you see the pectoralis measure 1 to 2 centimetres lateral to the pectoralis,
that's where you're gonna start seeing the nerves.
So the key is to try to preserve as much length as possible.
As long as it's oncologically safe, you can actually dissect those nerves through the
breast tissue to get some extra length, right?
The question is, are you going to connect the nerve to the skin just like showed in his
presentation or to the flap?
This is something that it's always being studied, also being studied.
There is a very important group to a big proponent on innervating the flap.
In nipple is perimastectomy, it's a completely buried flap.
I sometimes feel that innervating the skin in the nipple is better.
In that situation, you will need a nerve graft, whether you need an allograft or a
catavertic or an autograft from the seal nerve, but you need something to bridge that,
that bridge between the intercostal nerve and the nipporoa complex.
We can talk more later.
Thank you. Other questions?
I have a remark for the subcutaneous mastectomy.
It is well known and and and and German will agree that if you extend your incision to the
medial side that you have more risk of mastectomy, skin necrosis.
So I wonder, uh, do, because I do it like that, do you ever think of doing the anastomosis on
the on the thoraco dorsals? I only go for the thoraco dorsals if my IMV is
not good. The patient is radiated, but to your point,
I always have this dilemma because for my, uh, for the implant reconstruction,
we usually go midline and go lateral because you do preserve all the blood supply in the
nipperla complex. I think it helps to preserve the,
the, the blood supply for the nipple and on the deep flaps,
I'm always conflicted because you have to go more immediate to access the ribs.
If you, if my impression is if you put the, the arm open,
the access to the door because those vessels is extremely easy.
Maybe I should try that.
Yeah, really, because you, your approach is much more lateral,
you know. I, I, I was, I, I always did my anashemosis on
the, on the memories.
For robotic mastectomy, that's the way you have to do it.
You have to go to the intel and shoot the thoraco dorsal because,
you know, it's impossible to get to the internal memories,
yeah. Good point.
More questions? Another remark from me, I think we have no
control on the mastectomy, and I find it I work with many breast surgeons,
and each one has a different thing and most of the good cases you show in meetings are from
one or two breast surgeons because the most important part of the aesthetic outcome is the
mastectomy flap. However, in meetings they do not have sessions
on how to do mastectomy or the importance of mastectomy flap viability.
Even today's session that is about reducing the skin, but not about how to preserve the skin.
So I think that is going to be a big thing for us to get them to perform better mastectomies.
It's going to be a. Big challenge because it's not consistent.
It's really not, and it's funny because a lot of the surgeons now,
the breast surgeons are fellowship trained.
And they do a lot of new postparing mastectomy fellowship, but I'm sure you.
You have similar experiences it's it's very variable.
Our institution is a lot of ours has a lot of variability.
We have over almost 30+ breast surgeons, so on any given day you may end up with one that has
more experience doing nipple sparing, but to be honest, most of our breast surgeons don't do
nipple sparing, so our experience is fairly limited.
We do our mastectomies and uh so but I but we also have had a
learning curve. It's a process and another thing is that we use
plasma blade that it's really very harmless and and.
And we always push the residents not to pull just to know about how to treat the
tissues all those aspects.
I have a question for you.
When you do your stacked flaps, um, do you?
With the deep on top and the path below or the how do you,
what's your sequence?
Um, usually the deep is the larger flap, so we usually go integrate retrograde to the internal
memories, um, so the deep always goes to the integrate, uh,
internal memory and is sort of inferior pole, and then the pap usually goes above or under
the, uh, the deep for either more projection or upper polefulness and that usually goes to the
retrograde. um, we don't usually use to I am.
Kunon is a fantastic microsurge obviously Jim and everybody at uh in Barcelona.
The Thorocudoso vessels are very hard for us.
Um, it's, uh, it's a difficult sort of, uh, ergonomic access and oftentimes if it's delayed
and it's very radiated it is, uh, a little bit more challenging for us and,
um, I like to preserve it in case our flap dies and we still have the backup for the latissimus.
We, we must say that if we went into travel we go to Tarracosas and uh we don't consider LD as
the second choice.
And uh it's so that they sometimes they are quite tricky because especially we when it's
when you you do leave no transfer to thexilla, they are with radiation sometimes not they are
not so reliable but uh most of the time they work yeah you go up.
I must confess I'm an odd man out here.
I do use roosal quite regularly, especially when there is axillary dissection.
I don't go for IMA at all, and I think it's like everything else,
you get used to it and you have little nuances where you position the flap and get it.
OK, no more questions.
I think we can continue then. Thanks a lot, uh,
very much. Or next speak of
Barcelona. Uh, no, no, it's, it's, uh, sorry,
sorry, it says you guys, sorry, sorry, sorry.
Good morning, I'm Paul Roblin. I work at Saint Thomas's and Marlene's asked me
to um talk about how I, how I, how I raise an SAP flat.
How does this work? So no, no disclosures.
So the first thing is the patient. Um, I think Scap flaps can be a little tricky
in terms of which patient you choose, and I've become fussier over in the last,
I don't know, 1015 years.
Uh, what you want to have is a buttock which is nice and soft,
and there's a trade-off also between the height of the breast and the potential donorcy
deformity on the, on the buttock as well.
So ideally, I want to get a good height to make a good reconstruction.
You have to bear in mind that that may compromise the donorcy.
Obviously fat transfer can augment that later on, uh,
but you just really want a nice soft buttock which makes,
I think the dissection easier and you get a better result.
Um, I think choosing the, um, perforator is important.
I use an MRA scan, not everyone does.
Um, and the perforators as you can see on the bottom here,
and I'm, what I'm looking for is a lateral perforator, which is long and preferably large
as well. And the radiologist plots that over me.
If you see the bottom one, there's a dot in the midline and a dot where the perforator comes
out, and they measure that for me.
And that's then transferred into a grid, um, and the measurements are up from the coccyx
vertically and then transversely out from the midline.
And then that's transferred onto the patient.
Um, we used to raise these laps in the lateral position, but I do this pro now.
Um, we do quite a high proportion of bilaterals.
Um, and it's just easier for the posture as well.
And so. This is a schematic of how we do it.
So unilateral, so the patient will be supine to start with.
We do the mastectomy. Now then get the vessels ready,
get the chest ready. The patient's flipped over in the prone
position. And once the flap's been raised and the donor
site is being closed, we take the vessels off the table and dissect them with a microscope.
The patient sends supine again, uh, we shape the flap,
uh, and then do the micro and then put the flap in.
So that's a sequence to it, there are two turnings, but it doesn't really take too long
doing that. So it's just an example, this lady's got a
right, uh, immediate cancer mastectomy.
Uh, so once the mastectomy has been performed, I then redefine the pocket,
which is crucial, I think, to the end result.
And then I'll harvest the internal mammary vessels.
Often I go for the 4th rib. I'm not really bothered about which number,
but what I want is the rib, which is in the middle of the breast because it's going to make
the micro easier.
The pedicle of the SF can be quite short.
So I want to try and use that if there's a problem with that.
And also dissect from the rib to the ribs, who have a long length of internal mammary vessels.
So I always take the rib out.
Um, and raising the flap, ideally you want the scar in a high position which is transverse,
so it's hidden in the, in the panty line.
And again, we bear in mind the height we need for the reconstruction.
So, this just shows the raising of the flap, so the the coordinates are transferred on to the
patient. We confirm it with the Doppler, and it's
usually very accurate.
And then design the flap. So I've designed it so the the perforator is
lateral, um and I've measured the height of the breast, which I then transfer onto the bottom.
The skin, you maybe get 10 centimetres maximum on the bottom and probably less,
so you have to sham for above and below that to get the shape you want.
And then we champ for it, um, and I find champfing a lot easier inferiorly.
I get more volume and a um a less acute takeoff where superiorly it,
it is more abrupt. So there's the flat bra, and you can see
there's more fat inferiorly than than superiorly, it's no matter how I do it,
it always seems to work out like that.
And then the pedicle can be relatively short, but sometimes it's quite long.
And just a schematic of how I do it, so patients prone,
raise the flap. The perfect is lateral and again the chamin you
can see is better inferiorly.
So take the flap off and then rotate it 180 degrees and then go to the contralateral breast.
So I use the contralateral flap, and the reason for that is the champrin gives a better result
in terms of the reconstruction, but also the perforated is lying over the internal mammary
vessels. So again, if the if the vessel's short,
it facilitates the micro.
And pedicle dissection, so you go down to the fascia and there's a big confluence of vessels.
And I approach it from a superior lateral position, so you go through the parallel fibres,
and I really leave the perforator alone, just separate the muscle widely.
So try not to go down a small hole.
You get down to the fascia, open the fascia, and again,
try and spread widely again.
Don't get stuck in a small hole.
And when you get to that point, you'll find there's lots of branches coming off the main
vessel, and sometimes it's hard to know where the main vessel is,
but I kind of know now that the vessel's going to go straight in,
kind of in a medial direction.
She then come around, divide all of those branches.
And once we get low down, I use the microscope now to detect that.
It's safer and it's easier, and I also now try and get right onto the admin tissue of the
artery to, um, which, you know, allows better visualisation, and you can see if you get
beyond the confidence of the vessels, the artery is a good a good size match for the
internal mammary artery.
And then we dissect it off table and you can see if you get beyond that bunch of fat and
fibrous tissue, the artery is a good size, and usually the veins are always big.
Um, and I try not to dissect into that. It's it's like a ladder in there.
There's lots of branches and the fat and fibrous tissue keeps them in place.
I think one of the problems you can get is if you if you dissect the artery up a little bit,
uh, you can then have a small.
Ongoing artery and it can, I think it can bend very easily because as it is at the moment,
it's splinted by all the fibrous tissue.
Um, if you can't get down that far, then you can go proximal,
but the artery is smaller, but you can still do the anastomosis.
I think what we've done lately, um, is if you have like a V,
you can just de-roof the top of it and it opens it up like a book and then just makes the
artery anastomosis easier.
Um, so patients soup on again, so we shape the flap and get it all ready and then do the micro.
We always use the coupler and I think the SAPs in particular is very useful because the veins
can be very large.
And then we hand sew the tie, uh, hand tie the artery.
And then once that's done, you just put the flap in and do the final shaping and secure it.
What I don't want to be doing again because of the short pedicle is taking the flap in and out.
I just want to be able to put it in once.
So just some examples.
So just uh Skin sparing mastectomy, so this lady's quite a,
quite a short height on the breast, uh, and a soft bottom,
so she had a nice result from that.
Um, a bilateral, we do a lot of bilaterals now. I do these with Marlene,
and she, um, she does the genetics clinic.
And a typical patients slim, scars, bilateral reconstruction.
Um, also find with a lot of the patients, they tend to be fairly the younger patients and
slimmer. Um, and that the Scap is actually bigger or has
more projection than the other breast. So, in this lady,
we've done an augmentation as well on the right side.
And For the genetic genetics patients, um, we do most of these buried with an IMF incision,
but some need lifting, so there's two approaches for that.
One is to do a mastopexy, 3 months before the surgery, then to come back and you can do a
bilateral Scap reconstruction.
And this is Marlene's design, so instead of the, the batter the kind of batter wing incision
which goes across the breast, we just do a later one and then we slightly wider curved one
around the medial side.
And it gives a very nice result for a small lift.
Um, revisions, so mainly fat transfer and liposuction.
Uh, so just a couple of examples. This lady, uh,
had a bilateral implant reconstruction, uh, elsewhere, had a number of operations,
was quite unhappy.
Um, she's pretty slim, and had a bottom, but not a huge bottom.
So. Uh, we did a bilateral gap for her and then
augmented it with fat transfer later on. Again, you can see she's slightly short of
height and a bit of width on the left side.
I had a nice result in the end.
And this lady, uh, again from elsewhere, she'd had 11 operations for implant reconstruction,
um, again, very slim, um, a limited amount of tissue on the bottom.
So we did a bilateral Scap again with the skin paddle to start with.
Then we removed the skin paddle, and then I'll forget 23 or 4 revision surgeries with fat
transfer and reshaping and liposuction to give a reasonably nice result.
And donorcytes, problems with that dog ears, seroma contours,
dog ears, just try and avoid that with our design.
seroma, I've not got an answer for that, but we put drains in and the patients often go home
with drains. And the contour deformity, you can either get
some flattening or quite a dip sometimes.
So in the past I've always done an open, open revision of that.
So this is a lady who's not really suited for an SAP and predictably has a poor donor site.
Um, so what I do is, um, the epithelize the area of the dip.
And then I re lift the buttock on top of that.
And this can have a reasonably good result.
Uh, but more recently, and for, and for lesser defects, I tend to do a subcision scar release
and then fat transfer.
So kind of, I don't know what lessons I've learned, I,
I use an MRA scan so I'm trying to pick.
He perf, which will be lateral, um.
And then, as I said, what I'm trying to do then is put the perforator over the internal mammary
vessels over a long length, I'm trying to make the anastomosis easy so it's more reliable.
When I dissect, I open the muscles widely, I try not to get down a hole.
We use a scope at the bottom.
And then off table preparation of the vessels prior to the anashemosis.
And we used a couple of really all the time.
And What I want to do is just once the anasmosis is done,
just put the flap in. And there is a trade-off in terms of the height.
um, I tend to want to just get a nice reconstruction straight away,
so I think my donorcytes have got worse over the years.
Um, but the other way of doing that is a slightly smaller height and then fat transfer
for the breast afterwards.
Yeah, thank you. Sorry.
Thank you. The next speaker, Doctor Cumbalando.
He will talk about lumbar flap. He's probably one of the pioneers of this flap
in for Bersa construction, and I had the opportunity to be in one of your first ones in
Barcelona. Thanks a lot again for the invitation.
Uh, I'm gonna talk a little bit about the lap flap.
I'm just gonna give some details.
Uh, everybody is scared of doing a lap flap, and unfortunately it doesn't help much if
everybody keeps telling that I'm a special microsurgeon.
Uh, you know, you can do lap flaps, and I think there is a couple of tricks,
which also holds true for the SAPs, I think.
So if you look at the, the scenery out there and the deep flap is still the golden standard,
we don't do for every patient that we don't do a lead flap,
a lap flap. There is also other opportunities and
especially there's kind of a, uh, an indication for, for ASCAPS and,
and for laps, and it was mentioned before, it depends a little bit on the constitution of the
patient. So, but, uh, on top of that, I'm not the
inventor of the lap flap. The first lap flap was presented by Louis Duwa,
uh, and strangely enough, he didn't do any follow up of the,
uh, or other, uh, uh, series, so maybe it is a difficult flap.
So but we thought we're gonna dive into it and why?
Because there is a lot of patients out there like these kind of patients,
you see, these are either patients who had, uh.
Uh, problems, patients who are prosthetically crippled or even like this patient who you
could do a deep flap, but then the result of the deep flap would not be fantastic,
and she needs, essentially, she wants also a little bit of augmentation.
She doesn't want the prosthesis.
And if you look at these patients carefully, you will see that in most of these patients
unless they have a sagging buttock, but in most of these patients,
there is some excess tissue over here.
And in, in our culture it is also uh uh uh uh a habit to do the liposuction over there.
This is not the called the so-called saddlebags. So we,
we thought, can't we get use of this?
And then we started doing this, uh, SSA flaps and what is fantastic,
I think about this ASAP flap is the natural shape of the flap,
uh, of this slap flaps. If you do an ASAP flap,
you will see frequently if you don't bevel in in the right way and the patient has doesn't
have the right constitution that you have kind of a.
Uh, stepping off of your flap on the upper side or on the on the down sides.
And if you look carefully at, at the lumbar flap, this is really like an anatomical
prosthesis. The, the, the, the other thing is that the
amount of available tissue, there is always a lot of tissue available there.
The consistency and the shape of the flap, flap has a natural projection,
which we don't have with the deep flaps.
There is a possibility of neurotization and there is hardly any fat necrosis in lumbar
flaps. And there is a downward, obviously.
There's a learning curve. The technique is slightly technically more
demanding. There's a risk of seroma formation.
It's the same that you have with the ASA flap, and we addressed it a little bit.
And there is temporary some back pain possible, and you always have a visible scar.
You should tell the patient that the scar will be visible.
So, if you look at the CT scan and we do our CTs in prone position,
you can see that there is a huge amount of tissue over there and the uh lumbar flap,
uh, frequently has uh quite large perforators.
Unfortunately, when you go in, these perforators aren't that large as you presume
because over here this is the perforator, this is the aorta.
It should be a huge perforator, but the perforators are of decent size.
One of the things is we shouldn't go too deep in the beginning.
We followed our vessels too far, and then you risk of ending up in this zone where you have
the motor branches coming out and you get into trouble.
So in the beginning, we try to do as long as possible nowadays we don't do that anymore.
So we used to do the, the, the surgery starting in one,
doing one stage with the patient in lateral decubus position.
Now we changed to a three-stage procedure and essentially enough,
everybody thinks this is a burden and this is a hassle.
It goes faster.
The turning of the patient is not your issue. Turning of the patient is the problem of the
anesthesiologist and the nurses, and while they're doing their thing,
you can do your thing.
So we start with the patient in dorsal decubitus.
We do the breast and you accept the vessels, and then one extremely important point,
we always put an interposition graph and I will explain you.
We change the patient to ventral decubitus, we do the flap harvesting,
and then, uh, anastomosing on a side table.
And then uh we uh uh turn the patient again and we do just the anastomosis and the inserting of
the flap. So the graph is the key point in this whole
procedure, and I think it is also a key point in the SAP flaps because as has been addressed
by the previous speaker, there is, uh, if you do an SGAP flap,
there is uh frequently a huge discrepancy between the size of the vein and the acceptor
vein. And then if you do an, a, a decent uh
interposition graft, then you have to take care of this yourself.
You can't let it do by, by the residents, you know, you have to take care of,
of yourself. You can follow the, the, the graft into the
rectus muscle and then you. And you see that the size of the vessel tapers,
so you can really adjust the size of the vessels with your,
your flap pedicles so that you have an exact congruence of these vessels,
and I think this is the most important point in microsurgery.
So this is the harvesting of the of the of the graft.
59:59.850 --> 01:00:03.810 We did it while the patient was in in dorsal de pubitus.
01:00:04.010 --> 01:00:09.469 Do it yourself traction on the, on the pedicle, a clip which is mal positioned,
01:00:09.610 --> 01:00:13.159 uh, this all can end up in failure, and then you will start thinking,
01:00:13.290 --> 01:00:15.610 why is this, is this because this is such a difficult flap.
01:00:15.649 --> 01:00:19.679 No, it is because somebody harvested this interposition graft was not.
01:00:20.419 --> 01:00:23.919 Good at it. You just rinse this pedicle, put it aside,
01:00:23.979 --> 01:00:26.540 and you go on. Where is, what are the markings?
01:00:26.610 --> 01:00:29.260 The markings for the lumbar flap are quite easy.
01:00:29.580 --> 01:00:34.949 We do a CT scan and you can mark them, but the perforators are always on top of the iliac
01:00:34.949 --> 01:00:37.179 crest about 8 centimetres from the midline.
01:00:38.330 --> 01:00:41.290 You can you can almost palpate them. You can do them over there.
01:00:41.389 --> 01:00:45.969 They're always at 7 to 5 to 8 centimetres from the midline on top of the iliac crest.
01:00:47.429 --> 01:00:50.270 So we do the dissection, the dissection, we start medially,
01:00:50.479 --> 01:00:55.080 and one of the key points is that you first will encounter the clooney nerves.
01:00:55.199 --> 01:00:57.280 Once you encounter the clooney nerves, this is a landmark.
01:00:57.399 --> 01:01:01.709 You see the clooney nerves, you know that your birth rate is going to be behind about 1 to 2
01:01:01.709 --> 01:01:04.790 millimetres. At that point, you take the microscope.
01:01:05.439 --> 01:01:08.199 We always take the microscope. The section is much easier,
01:01:08.270 --> 01:01:12.050 it goes faster, and we only dissect for about 34 centimetres.
01:01:14.179 --> 01:01:20.800 So we raise the flap and you can see that you can really get in thin patients quite large
01:01:20.800 --> 01:01:25.879 flap and you have to be careful not to overharvest because you overharvest sometimes
01:01:25.879 --> 01:01:29.239 you really have to resect. You have to resect part of the of your flap and
01:01:29.239 --> 01:01:32.120 throw it away and obviously the more flap that you harvest,
01:01:32.159 --> 01:01:33.909 the more donor side effect that you have.
01:01:36.370 --> 01:01:40.050 There is the possibility of harvesting these long sensate nerves,
01:01:40.090 --> 01:01:42.169 the clooney nerves. In the beginning we thought because these
01:01:42.169 --> 01:01:45.479 clooney nerves are are quite important and they're quite thick,
01:01:45.929 --> 01:01:49.250 and we thought we're going to provoke a sensate deficiency in the buttock,
01:01:49.290 --> 01:01:52.610 but it doesn't, it doesn't happen. I don't know why there is a sensate,
01:01:52.629 --> 01:01:56.969 a little sensate deficiency, but it's on top of your scar and there is no problems with the
01:01:56.969 --> 01:02:00.570 buttock, but you have very long nerves. This is the pedicle you can see.
01:02:00.649 --> 01:02:03.449 We don't harvest that pedicle that long. It's a very short pedicle.
01:02:03.909 --> 01:02:06.800 You can augment it by dissecting a little bit further, but in the end,
01:02:06.830 --> 01:02:10.520 you will end up with a pedicle of about 67 centimetres at maximum.
01:02:10.800 --> 01:02:12.669 So better to harvest it a little bit shorter.
01:02:13.600 --> 01:02:18.989 And do this interposition graft. This interposition graft allows a shortening
01:02:18.989 --> 01:02:22.780 dissection of the donor side because as, as well as with the S gap,
01:02:22.790 --> 01:02:27.260 as with the lumbar flap, the dissection starts in the depth there it becomes tricky.
01:02:27.870 --> 01:02:31.510 So if you shorten your pedicle lengths and you put them into position graph,
01:02:31.590 --> 01:02:33.389 you avoid these kind of problems.
01:02:33.820 --> 01:02:37.179 It lengthens your pedicle, gives you a size match of the anastomosis,
01:02:37.300 --> 01:02:41.429 and in the end it gives you a safer outcome. Everybody thinks that by doing an extra
01:02:41.429 --> 01:02:45.959 anastomosis, you augment the risk of failure of your flap.
01:02:46.139 --> 01:02:50.100 I can assure you that once we started doing these interposition graphs,
01:02:50.139 --> 01:02:52.120 our failure rates dropped dramatically.
01:02:54.100 --> 01:02:56.810 So while they're turning the patient, this is not lost time,
01:02:57.020 --> 01:03:00.439 while they're turning the patients you do and uh the the.
01:03:01.000 --> 01:03:05.750 Anastomosis of this uh interposition graph and this anastomosis has to be meticulous.
01:03:05.830 --> 01:03:08.739 It has to be perfect from the first time. There is no,
01:03:08.830 --> 01:03:12.389 no way that there can be leakage. You have to test it and it has to be perfect
01:03:12.389 --> 01:03:16.219 from the first time. Most of the time we do it with 100.
01:03:17.110 --> 01:03:19.919 So you can do the nervi looney, you can, you have, uh,
01:03:19.929 --> 01:03:23.040 enough length of, of these nerves to do both a medial and a nerve,
01:03:23.129 --> 01:03:25.610 and a lateral nerve coaptation if you want.
01:03:25.989 --> 01:03:29.159 We do it just with the, we don't, we, we don't have the money available like,
01:03:29.169 --> 01:03:33.250 uh, they have in the United States, so we don't have all these kind of fancy interposition
01:03:33.250 --> 01:03:36.090 things. We do it just with a, a vein, uh, a vein graft
01:03:36.090 --> 01:03:39.290 and, and a cuff. So, I'm just gonna show you one case.
01:03:39.370 --> 01:03:41.360 This is a patient 52 years old.
01:03:41.649 --> 01:03:43.370 Somebody did to her and, uh.
01:03:44.050 --> 01:03:47.709 Bilateral mastectomy without without proposing any reconstruction,
01:03:47.760 --> 01:03:49.520 so obviously the patient regret it.
01:03:50.639 --> 01:03:53.439 It doesn't have that much abdomen and this is the result.
01:03:53.629 --> 01:04:00.350 Bilateral in two stages, uh, uh, uh, lap flap, bilateral nip
01:04:00.350 --> 01:04:03.520 reconstruction on the local anaesthesia, no other corrections,
01:04:03.669 --> 01:04:05.229 no liposuction, no lipofilling.
01:04:05.909 --> 01:04:08.489 And this is a results pre and postoperative.
01:04:09.949 --> 01:04:12.060 And this is the donors side scar. As you can see,
01:04:12.139 --> 01:04:15.500 the donor site scar is on top of the, of the, of the,
01:04:15.550 --> 01:04:18.340 of the pants. It, it depends a little bit on which kind uh
01:04:18.340 --> 01:04:21.050 kind of pants you use most most of the time it will be on top.
01:04:22.010 --> 01:04:25.219 And you have to take extreme care because this is a two-stage procedure.
01:04:25.260 --> 01:04:29.149 You have to take extreme care that you have an uh a symmetrical scar.
01:04:29.580 --> 01:04:32.620 You really have to take care of that because if you have an asymmetrical scar,
01:04:32.699 --> 01:04:36.379 it is, uh, horrendous. So in conclusion, in a lot of patients,
01:04:36.459 --> 01:04:39.770 not in all of them, we do all kinds of flaps, but in a lot of patients,
01:04:39.860 --> 01:04:44.209 the lap flap became the second choice, uh, uh, for autologist breast reconstruction.
01:04:44.340 --> 01:04:45.340 Thanks a lot.
01:04:53.129 --> 01:04:56.409 Now we would ask, give me a second.
01:04:58.000 --> 01:05:03.020 Oh my God. Yeah, um.
01:05:06.199 --> 01:05:11.300 Van, sorry, I, my, my eyesight is bad to talk about 5 flaps.
01:05:11.399 --> 01:05:11.969 Thank you. Thank you.
01:05:11.979 --> 01:05:18.620 Um, thanks Marlene, Joe and Jian for the invite and uh uh
01:05:18.620 --> 01:05:22.409 congratulations on your 10th anniversary. It's fantastic to be here.
01:05:23.199 --> 01:05:25.560 Uh, the topic is thigh flaps.
01:05:26.300 --> 01:05:29.570 And there are 3 main thigh flaps we'll discuss.
01:05:30.020 --> 01:05:33.139 And of course, uh, grizzly space flaps, such as the tug flap,
01:05:33.300 --> 01:05:38.169 dog flap. The pap flap and the LTP flap, the lateral type
01:05:38.169 --> 01:05:43.020 perforator flap. That said, uh, autologous reconstruction,
01:05:43.110 --> 01:05:46.350 all of us in this room will agree is the best form of reconstruction,
01:05:46.429 --> 01:05:52.469 most durable, most aesthetic, and abdominal flaps are the best flaps because they give
01:05:52.469 --> 01:05:55.300 large volume, the size, the consistency.
01:05:55.600 --> 01:05:59.139 And it also adds to the aesthetic enhancement of the abdomen,
01:05:59.229 --> 01:06:00.939 so they are the first choice.
01:06:01.270 --> 01:06:06.750 In some patients who have had liposuction or abdominoplasty or previous DF flaps or
01:06:06.750 --> 01:06:12.110 inherently less abdominal adiposity, we need to look at other flaps and thigh and lower back
01:06:12.110 --> 01:06:13.590 and gluteal flaps.
01:06:14.310 --> 01:06:19.360 The ones which come to the rescue with regards to the Tigh flaps.
01:06:19.969 --> 01:06:24.040 The top flap is my preferred choice. It's a micocutaneous flap.
01:06:24.169 --> 01:06:27.580 That's one flap. You don't have to look for perforators,
01:06:27.610 --> 01:06:32.449 and it's a quick race and it can be done in a supine position and it's very predictable
01:06:32.449 --> 01:06:35.320 anatomy. However, it has a short pedicle and a small
01:06:35.320 --> 01:06:40.830 calibre. The perforator pure here would prefer pap flap,
01:06:41.270 --> 01:06:47.389 and uh it has a long pinnacle, good calibre, and uh one of the problems is the scar might
01:06:47.389 --> 01:06:51.229 have to be pushed in lower because the perforator location could be lower in some
01:06:51.229 --> 01:06:53.790 patients. And positioning of the patient.
01:06:53.959 --> 01:06:56.870 You can't do it in a supine person you need to sit between the legs.
01:06:57.360 --> 01:07:02.469 And uh LTP flap in my hands is an opportunistic opportunistic flap.
01:07:02.719 --> 01:07:07.679 It's an easy race, longer, large calibre, but the donor site has much to be desired.
01:07:09.360 --> 01:07:13.419 So that said, first we'll look at the transfers up a restless flap,
01:07:15.850 --> 01:07:18.969 which is first given to us by Zora Arne and 20 years ago,
01:07:19.219 --> 01:07:20.860 and Thomas Schler refined it.
01:07:21.300 --> 01:07:26.340 And the indications are small breasts, non-availability of abdominal tissue as we
01:07:26.340 --> 01:07:29.739 discussed, and there has to be adequate thigh adiposity.
01:07:30.639 --> 01:07:36.739 There are a few points here to note. The skin paddle has to be slightly lower.
01:07:37.030 --> 01:07:41.110 It's very important that these trans slabs don't take the paddle too high because the skin
01:07:41.110 --> 01:07:45.350 very close to the crease does not have any fat. You'll only increase the size of the skin
01:07:45.350 --> 01:07:47.820 paddle and create problems with your donors.
01:07:48.879 --> 01:07:55.370 In a tug flap, as with pap flap, most of the tissue is taken from the posterior part,
01:07:55.659 --> 01:08:00.219 posterior to the aggressalis, and that's where the posterior thigh and the poster upper thigh
01:08:00.219 --> 01:08:01.570 is where the fat comes from.
01:08:01.860 --> 01:08:08.100 And inferior recruitment of fat along the skin edge below the membranous layer of the
01:08:08.100 --> 01:08:11.260 superficial fascia is very important. It may not seem like much,
01:08:11.300 --> 01:08:15.540 but it will be a good percentage of the flap volume because these are very small flaps.
01:08:16.168 --> 01:08:22.329 And it is a melon slice and a crescentic one, and it easily cones and the dog ear becomes a
01:08:22.329 --> 01:08:25.039 nipple. For small breast, it's ideal.
01:08:25.929 --> 01:08:31.338 And I'm a systems person. There are 8 steps in my planning of a flap,
01:08:31.458 --> 01:08:34.729 tug flap, and it starts with the caudal extension.
01:08:34.749 --> 01:08:37.298 It's so important to recruit that little bit of fat there.
01:08:37.700 --> 01:08:40.620 And then the next one is the anterior flap elevation.
01:08:40.660 --> 01:08:46.939 This is crucial here, not to overharvest this tissue over the femoral triangle until you come
01:08:46.939 --> 01:08:52.180 up to the syphalous vein, you need to be very careful, just keep superficial and go right
01:08:52.180 --> 01:08:56.399 down soon after causing the syphanous vein. You go right down to the adductofascia,
01:08:56.569 --> 01:08:59.339 and that forms the vascular basis of this flat.
01:08:59.609 --> 01:09:04.049 The adductofascia splits and inverts the aggressalis muscle and the connection between
01:09:04.049 --> 01:09:07.680 the grassless muscle, the adductofascia, and the fat is so important.
01:09:07.930 --> 01:09:10.560 So it's important to cut the fascia somewhere there.
01:09:12.290 --> 01:09:16.649 Next is division of the aggress. Step 3, do not take long lengths of muscle.
01:09:16.709 --> 01:09:19.560 It's not useful. It's just a trophies.
01:09:20.009 --> 01:09:25.120 And then this is a crucial bit where you recruit the real flap.
01:09:25.330 --> 01:09:28.910 This is where you harvest the fat from the upper posterior thigh.
01:09:29.129 --> 01:09:33.290 It's important to make sure that you don't cross the posterior mid axial line because
01:09:33.290 --> 01:09:35.490 that's where the posturecutaneous nerve of thigh is there.
01:09:37.089 --> 01:09:42.729 And the division of the proximal groceli and the pedicle dissection and detachment.
01:09:42.939 --> 01:09:48.060 Here the leg has to be kept straight and the adducta relaxed and the ducta retracted
01:09:48.060 --> 01:09:52.720 laterally. You have a crescentic piece of tissue.
01:09:52.890 --> 01:09:56.810 You can use it three ways. The full cone is what I use mostly because
01:09:56.810 --> 01:10:00.310 there's a self-selected group of patients with smaller per breasts.
01:10:00.770 --> 01:10:07.149 If the breast is small and tautic, half cone, don't just the horns are switched to the muscle,
01:10:07.490 --> 01:10:10.879 and in a very tautic breast, small breast where there's no upper pole,
01:10:11.049 --> 01:10:12.410 you can just leave it unconned.
01:10:13.089 --> 01:10:16.600 And intercostal perforators are our preferred choice.
01:10:16.720 --> 01:10:20.100 Over 75% of our patients will use the intercostal perforator.
01:10:20.279 --> 01:10:25.959 We'll dig it into the pectoralis major and get a small length even if it's been charred at the
01:10:25.959 --> 01:10:29.830 surface of the pectoralis major because this makes the anasomosis very easy,
01:10:29.879 --> 01:10:33.390 the calibre match and also it is the reach.
01:10:34.319 --> 01:10:39.660 And this is an example of a patient who has had a flap.
01:10:39.910 --> 01:10:45.060 In patients with just the lower pole and not much of an upper pole,
01:10:45.229 --> 01:10:49.419 but you need to give a smooth transition because tug flap is a thick flap.
01:10:49.669 --> 01:10:55.669 So to transition that it's good to have lipo, the pectoralis major,
01:10:55.709 --> 01:11:00.939 which you can do prior to placing the flap so as to give a smooth take off.
01:11:01.649 --> 01:11:06.490 And uh in some patients we can do secondary lafiing pre-medicated because these are smaller
01:11:06.490 --> 01:11:09.270 flaps. This patient had a dip and of course a tug flap,
01:11:09.310 --> 01:11:11.180 which is not a match in size.
01:11:11.470 --> 01:11:15.419 And in there's a vascular matrix transfer which Kundrad has mentioned,
01:11:15.629 --> 01:11:17.910 you can pump it with fat and make it bigger.
01:11:18.959 --> 01:11:24.160 Donnocyte, the thigh donnocytes are more complication prone than the abdominal donnocyte,
01:11:24.560 --> 01:11:30.240 and the usual problem is the posterior wound deheins because that's where the patient puts
01:11:30.240 --> 01:11:33.169 enormous amount of pressure when they are sitting very early post-op period.
01:11:33.720 --> 01:11:37.879 So it is important to focus on this closure while doing this,
01:11:37.930 --> 01:11:43.850 and it is a nuisance, but I think the operative surgeon, the senior surgeon should do this and
01:11:43.850 --> 01:11:49.359 have to splint the wound with multiple switches and also we use the prene or liquiband tape,
01:11:49.569 --> 01:11:51.959 which gives extra strength to the wound.
01:11:52.770 --> 01:11:58.120 It is important to avoid the postercuenous nerve, and neuroma here is a big nuisance and
01:11:58.120 --> 01:12:00.620 it's quite crippling for the patient whenever they sit down.
01:12:01.729 --> 01:12:04.279 Another problem with these slaps are the scar migration.
01:12:04.339 --> 01:12:07.149 This is something I have not been able to predictably control,
01:12:07.399 --> 01:12:12.799 and we need to counsel this patient, especially patients with lax tissue and very lax skin.
01:12:14.189 --> 01:12:17.819 medial thigh contour defects are a problem with slim patients.
01:12:18.049 --> 01:12:21.020 So this is nothing much you can do to address other than lipofilling,
01:12:21.029 --> 01:12:24.189 but you can't find enough fat in these patients to fill it with.
01:12:25.009 --> 01:12:29.540 So our strategy in these flaps are not to overharvest, use primary or secondary
01:12:29.540 --> 01:12:33.049 lipofilling, use two flaps if necessary for one breast.
01:12:33.500 --> 01:12:35.410 Do not cross the mid-ingranal point.
01:12:35.660 --> 01:12:38.250 Do not overharvest the femoral triangle.
01:12:38.500 --> 01:12:43.620 Do not cross the postre axial line of the inferior gluteal crease to avoid the
01:12:43.620 --> 01:12:45.049 postrecutaneous ner thigh.
01:12:46.970 --> 01:12:51.629 And in patients with large breasts with limited thigh, twin flaps are better.
01:12:51.879 --> 01:12:53.189 It limits the harvest.
01:12:53.439 --> 01:12:56.029 You don't have to overharvest the flaps.
01:12:56.339 --> 01:13:00.959 But the problem here is the recipient vessels, because these are short pedicles and so you
01:13:00.959 --> 01:13:03.520 need to have recipient vessels and of course the.
01:13:03.709 --> 01:13:07.009 Access is available to us. It gives ample opportunity,
01:13:07.180 --> 01:13:13.339 but here the anterior branch comes in for the 2nd flap because the orientation of the flaps
01:13:13.339 --> 01:13:14.410 are going to be difficult.
01:13:14.620 --> 01:13:19.299 And when you start considering twin flaps, you need to think of recipient how are you going to
01:13:19.299 --> 01:13:20.339 orient the flaps.
01:13:22.040 --> 01:13:26.100 The best orientation is the curvature is parallel to each other,
01:13:26.319 --> 01:13:29.819 so one flap could be conned like that and one flap for the lower part.
01:13:30.149 --> 01:13:35.350 And if you're going to do this, the perforators so the vessels will be pointing the opposite
01:13:35.350 --> 01:13:38.310 way. This will go to the contralateral flap will
01:13:38.310 --> 01:13:42.029 connect to the internal mammary, ipsilateral flap has to go this way.
01:13:42.540 --> 01:13:46.060 If there is an adductor branch, of course, you can use the director branch to perfuse the
01:13:46.060 --> 01:13:49.779 second flap. If not, you need to use anti-grade retrograde
01:13:49.779 --> 01:13:55.020 is not very good aesthetically, because the curvature of two flaps are not matching each
01:13:55.020 --> 01:13:59.580 other. This is an example of the first one, a corn
01:13:59.580 --> 01:14:04.819 flap, but in these cases, you need to extend the flap with main graphs or pedicle graphs.
01:14:05.910 --> 01:14:11.620 And this is a case where we had used a post-op result, and you can see by not overharvesting
01:14:11.620 --> 01:14:16.790 the ice scars can be kept reasonably high and sky donor site is reasonably acceptable.
01:14:17.520 --> 01:14:23.910 In patients with wide breasts and large breasts and limited abdominal adiposity at one side,
01:14:24.100 --> 01:14:28.080 thigh flaps come in handy to go along with the deer flap,
01:14:28.120 --> 01:14:29.549 and we spoke about this.
01:14:29.799 --> 01:14:34.439 I tend to place the deer flap upside down, delis and the cranial end of the deer reel is a
01:14:34.439 --> 01:14:37.640 good match for the grailli and that.
01:14:38.404 --> 01:14:44.365 This is a result of a patient who had this is a very good way of doing one stage reconstruction
01:14:44.365 --> 01:14:45.464 of the nipple and so on.
01:14:45.765 --> 01:14:52.125 And you can also aesthetically modify the shape of the breast by placing the flap in the centre
01:14:52.125 --> 01:14:56.084 like this for a pert breast or lower down for a tortic breast,
01:14:56.165 --> 01:15:00.075 so it allows lots of advantages it has.
01:15:00.365 --> 01:15:04.884 So with a tug flap, you can use a tug flap only. You can do a contralateral reduction and make
01:15:04.884 --> 01:15:06.015 the other breast smaller.
01:15:06.479 --> 01:15:12.029 You can use twin tugs for one flap, one breast, add lipofilling secondarily primarily,
01:15:12.160 --> 01:15:13.589 or even add an implant.
01:15:14.990 --> 01:15:21.660 Next, it's a path flap, and this is Bob Allen taught us about this about 10 years ago.
01:15:21.830 --> 01:15:28.669 It was discovered serendipitously in Mexico when there was a perforator course and Bob
01:15:28.669 --> 01:15:33.549 did this and maybe 5 weeks later he had done 20 cases and he published it.
01:15:34.009 --> 01:15:37.060 And so this is an excellent flap.
01:15:37.569 --> 01:15:43.970 It takes a tissue very similar to the tug tissue, and the perforator is from the first
01:15:43.970 --> 01:15:47.810 perforator perforating artery of the proffemoris, and it goes through the ductor
01:15:47.810 --> 01:15:53.580 magnus, and it is a perforator flap, of course, you need to price the muscle apart to get the
01:15:53.580 --> 01:15:55.919 flap. So that's why I try to avoid it.
01:15:56.209 --> 01:15:59.370 And sometimes these perforators are quite low from the in.
01:15:59.910 --> 01:16:02.580 Up to 12 centimetres, then you need to chase the perforator.
01:16:02.790 --> 01:16:04.939 That's when the scar starts going low.
01:16:05.149 --> 01:16:11.109 But more recent work from Andrea Figues from Sardinia, he showed with the last series that
01:16:11.109 --> 01:16:15.270 if you capture the perforator in the fat extension, that's good enough and there is very
01:16:15.270 --> 01:16:18.060 little fat necrosis. It doesn't have to be in the skin panel,
01:16:18.310 --> 01:16:24.950 and this has made it easier to migrate the scar upwards, and this is the kind of orientation I
01:16:24.950 --> 01:16:29.580 use now. And this is a result of a pap flap with a
01:16:29.580 --> 01:16:32.779 nipple sparing mastectomy and a fairly high scar.
01:16:34.859 --> 01:16:38.390 So, tug versus pap, tug gives slightly more volume, I think,
01:16:38.479 --> 01:16:43.509 and it's faster elevation, certainly easier positioning and consistent scar location.
01:16:43.879 --> 01:16:49.279 Uh, PA flap has a longer pedicle, larger calibre, and certainly less lymphedema risk
01:16:49.279 --> 01:16:50.799 because you're slightly more posterior.
01:16:51.720 --> 01:16:56.950 And the LTP flap, the final flap, this is uh Seania Tunder popularised this.
01:16:57.240 --> 01:17:04.220 It's a septocutaneous tenta fascia later flap, and uh the It is limited in my experience to
01:17:04.220 --> 01:17:09.129 prominent patients with prominent riding bridge deformities where the outer thigh is quite full
01:17:09.459 --> 01:17:13.689 and the perforators are quite consistent. Many perforators,
01:17:14.020 --> 01:17:17.419 antidis expand to lateral border of the.
01:17:18.120 --> 01:17:24.759 and at the pubic bone level there are multiple perforators and uh this is a patient so for
01:17:24.759 --> 01:17:28.640 completion's sake, I'm adding this flap, um, a large breast,
01:17:29.000 --> 01:17:33.200 bilateral LTP flaps and placed in and uh.
01:17:33.500 --> 01:17:37.729 This is a result, but the donor site has much to be desired.
01:17:37.750 --> 01:17:43.330 This is after a stage of lipofilling and liposuction, so this has been a problem in our
01:17:43.330 --> 01:17:46.890 hands. Certainly the Maastricht group has perfected
01:17:46.890 --> 01:17:52.330 this, and they seem to use this much more than the other medial thigh flaps.
01:17:53.459 --> 01:17:58.680 So in selected patients with limited abdominal adiposity, thigh flaps provide an alternative
01:17:58.680 --> 01:18:01.959 solution. Volume available is limited in most cases and
01:18:01.959 --> 01:18:03.750 may require adjunctive measures.
01:18:04.279 --> 01:18:09.560 Shape of these slaps, particularly the width, are more limited in comparison to DFP,
01:18:09.799 --> 01:18:14.859 so the footprint of the breast to match it, you might have to add other contouring procedures.
01:18:15.319 --> 01:18:19.470 Donor morbidity and contour defects are more prevalent in thigh flaps,
01:18:19.879 --> 01:18:25.220 but they are Very good 2nd line flaps for breast reconstruction.
01:18:25.709 --> 01:18:26.709 Thank you very much.
01:18:32.580 --> 01:18:38.270 The the last speaker, Doctor Mark Cheverian is going to talk about inserting of the delayed
01:18:38.270 --> 01:18:39.379 flat reconstruction.
01:18:41.689 --> 01:18:46.379 Thank you and uh A lot of this has been covered by the other speakers,
01:18:46.509 --> 01:18:51.180 some really fantastic, you know, results from autologous reconstruction.
01:18:52.040 --> 01:18:55.109 Um, so I'm gonna talk about the inset the delayed flap,
01:18:55.200 --> 01:19:01.040 uh, no disclosures for this talk, and Much of the earlier talks were on,
01:19:01.229 --> 01:19:05.049 uh, autonomous reconstruction after immediate, uh, you know,
01:19:05.160 --> 01:19:07.689 bilateral nipple sparing breast reconstruction, and you know,
01:19:07.759 --> 01:19:14.359 this is a lovely patient population to get some tremendously good
01:19:14.359 --> 01:19:17.959 cosmetic results. Um, if you have a good breast surgeon that can
01:19:17.959 --> 01:19:22.080 do a nice nipple sparing mastectomy and leave generous flaps,
01:19:22.399 --> 01:19:26.600 you can get some exceptionally good results and, and very satisfied patients.
01:19:28.020 --> 01:19:35.020 We have to deal with radiation though, and um uh one really elegant way of managing this
01:19:35.020 --> 01:19:37.970 has been a preoperative radiation.
01:19:38.180 --> 01:19:45.129 So um this is relatively new to the US at MD Anderson we've we did the first trial,
01:19:45.209 --> 01:19:48.459 and we did a randomised control trial which we have completed and published,
01:19:48.529 --> 01:19:51.330 and now we're on our, our second randomised control trial.
01:19:51.740 --> 01:19:56.310 And you know, these sorts of results we really could not achieve uh with uh conventional
01:19:56.310 --> 01:20:00.390 techniques of tissue expander, uh, and conventional delayed reconstruction,
01:20:00.399 --> 01:20:05.379 it really uh kind of um combines the advantages of immediate reconstruction,
01:20:05.390 --> 01:20:11.350 uh, uh, with, um, uh, you know, the need for, for radiation therapy and and and those
01:20:11.350 --> 01:20:15.459 considerations. So realistically, this is what we're dealing
01:20:15.459 --> 01:20:20.290 with, uh, in the large part, and, um, half of our patients at MD Anderson that get,
01:20:20.339 --> 01:20:24.180 um, mastectomy, get a total mastectomy and no immediate reconstruction,
01:20:24.220 --> 01:20:26.620 mainly because they have pretty big bad tumours.
01:20:27.410 --> 01:20:31.379 Um, Anderson is, is, is world famous for its radiation therapy,
01:20:31.390 --> 01:20:35.830 and it really does leave a lot of injury to the chest wall,
01:20:36.060 --> 01:20:40.319 um, particularly in this photograph on the right of a patient that's that's lost her
01:20:40.319 --> 01:20:41.509 reconstructions.
01:20:42.020 --> 01:20:45.700 The other issue of patients that have comorbidities that didn't allow them to have a
01:20:45.700 --> 01:20:47.189 tissue expander placed.
01:20:47.560 --> 01:20:49.660 Uh, you know, everything is bigger in Texas. We have,
01:20:49.779 --> 01:20:52.299 we have big patients with big abdomens.
01:20:52.879 --> 01:20:56.729 And then they come to us for delayed reconstruction, and then on the left,
01:20:56.810 --> 01:20:59.720 many of our patients, uh, subsequently developed lymphedema,
01:20:59.970 --> 01:21:04.970 uh, which we're managing, and the majority of my patient population are getting um abdominal
01:21:04.970 --> 01:21:07.290 flaps, uh, with lymph node transfers.
01:21:08.819 --> 01:21:13.939 So how can we make our, you know, immediate reconstructions look as good as our delayed
01:21:13.939 --> 01:21:19.740 reconstructions, such as in this case, whereby um did an immediate delayed reconstruction at
01:21:19.740 --> 01:21:23.990 the same time, with some nuances we can get closer, it's not perfect,
01:21:24.060 --> 01:21:27.089 they don't look the same, but, but, you know, we can get pretty close.
01:21:27.660 --> 01:21:31.450 And there are numerous tips and tricks, and I by no means have come up with,
01:21:31.540 --> 01:21:33.419 with all of these. I've learned them.
01:21:33.770 --> 01:21:36.890 Through my training, through my mentors, um, and, uh,
01:21:36.899 --> 01:21:41.729 but by putting them together, I think it does give you a working scaffold for how to,
01:21:41.759 --> 01:21:43.890 to, to manage these complex patients.
01:21:44.890 --> 01:21:47.250 The first is something that I'm sure that we all practise,
01:21:47.330 --> 01:21:50.459 but I, I just want to make this point because I do see this a lot.
01:21:50.910 --> 01:21:53.589 Firstly, deepithelialis the inferior mastectomy skin flap,
01:21:53.620 --> 01:21:57.060 that gives you that uh lower central projection, which is really important.
01:21:58.009 --> 01:22:02.279 Uh, the second and combined aspect of this is really be very thoughtful about where to um
01:22:02.279 --> 01:22:07.490 site the IMF, and, uh, certainly, you know, you have two choices.
01:22:07.569 --> 01:22:12.310 One is, uh, to commit to a, to an incision that is higher,
01:22:12.649 --> 01:22:16.089 um, and then you can subsequently lower that once the flap is inset.
01:22:16.609 --> 01:22:20.089 And I like to do that where a patient has a toutic breast and to,
01:22:20.209 --> 01:22:23.689 to, to match the, uh, the other breast, particularly in the unilateral setting.
01:22:24.089 --> 01:22:27.979 You have to be quite aggressive at thinning that skin so it will fold over on itself.
01:22:28.189 --> 01:22:30.120 If you don't do that, it doesn't look right.
01:22:30.490 --> 01:22:34.560 And the other is in a patient with minimal ptosis or that is getting a bilateral,
01:22:34.770 --> 01:22:39.560 um, you can close the abdomen fully first and then decide where to deepithelialize.
01:22:39.770 --> 01:22:44.970 And again, these are common techniques, but it is much easier to lower and malplace IMF than
01:22:44.970 --> 01:22:50.509 to try and raise it. This is a technique that I learned from uh one
01:22:50.509 --> 01:22:53.430 of my mentors, Mr. Ramakrishnan, and this indeed is one of his
01:22:53.430 --> 01:22:59.399 photographs on the, on the right side from publication and um I learned this on fellowship
01:22:59.399 --> 01:23:05.350 with him, and it has really changed my practise. So you can take quite a considerable amount of
01:23:05.350 --> 01:23:10.379 fat from under the scarpus fascia, cephalad uh to your uh to your flap,
01:23:10.709 --> 01:23:14.149 um, and this really helps with that upper medial inset.
01:23:14.689 --> 01:23:21.600 And using this technique and some modifications, I have to do very few um stack pack deeps to
01:23:21.600 --> 01:23:24.160 be able to reconstruct that upper pole.
01:23:24.490 --> 01:23:29.370 The other thing that it helps with is the abdominal closure because it really helps to to
01:23:29.370 --> 01:23:34.259 match the height of the abdominal closure with the um the inferior closure.
01:23:35.339 --> 01:23:37.939 This is a small point, but I, I think it is important.
01:23:38.060 --> 01:23:41.729 So you know, in the radiated breast, the uh pre-pectoral fascia,
01:23:41.899 --> 01:23:47.459 that same plane that we now do our um sub-pectoral breast augmentations in can get
01:23:47.459 --> 01:23:48.500 very fibrotic.
01:23:49.250 --> 01:23:54.649 And when you're raising your mastectomy skin flaps, I often see that they're raised onto the
01:23:54.649 --> 01:23:57.850 muscle. And if you do that, that very fibrotic layer
01:23:57.850 --> 01:24:01.279 does affect the ability of that mastectomy skin flap to open up.
01:24:01.609 --> 01:24:04.609 So it is a defined layer. I like to leave it in the radiated setting on
01:24:04.609 --> 01:24:08.049 the chest wall, and then we get a much more pliable mastectomy flap,
01:24:08.060 --> 01:24:11.490 and you can see the difference when you follow these patients up longer term.
01:24:12.509 --> 01:24:15.839 This is a nuance that may be a little controversial, but I,
01:24:15.910 --> 01:24:20.709 I, I do like to employ this, and I learned this from my pre-pectoral breast reconstructions
01:24:20.709 --> 01:24:26.859 whereby I do uh raise a small plane of the pectoralis muscle to address that upper pole,
01:24:27.060 --> 01:24:30.729 so you don't get that stuck on appearance with the expander and then the implant.
01:24:30.750 --> 01:24:33.779 I found subsequently you have to do less autologous fat grafting.
01:24:34.189 --> 01:24:38.910 So I lift up a small uh lip of the the muscle that's obviously adherent to the mastectomy
01:24:38.910 --> 01:24:42.450 skin flap. I go where the muscle fibres change direction
01:24:42.450 --> 01:24:47.009 between the clavicular and the sternal heads, and this really does improve the upper pole.
01:24:47.290 --> 01:24:52.169 Um, the patients don't animate uh when they contract and it has reduced the amount of
01:24:52.169 --> 01:24:54.040 revisions I've had to do to the upper pole.
01:24:54.250 --> 01:24:56.970 So it, it's a nuance that I've found to be very helpful.
01:24:58.100 --> 01:25:01.569 Again, a little controversial, but I, I want to discuss it all the same.
01:25:02.419 --> 01:25:05.290 So particularly if patients had a modified radical mastectomy,
01:25:05.459 --> 01:25:10.220 there is a lot of loss of volume in the axilla, and in the immediate setting,
01:25:10.379 --> 01:25:13.290 particularly if a patient has not had an axillary lymphadenectomy,
01:25:13.540 --> 01:25:16.410 absolutely we can treat the flap like an implant.
01:25:16.899 --> 01:25:20.129 But in the delayed setting, the flap is, is not like an implant,
01:25:20.140 --> 01:25:24.250 and if we orientate the flaps vertically, um, as is,
01:25:24.299 --> 01:25:28.419 is a fashion, and particularly folding that lower portion of the breast under.
01:25:28.979 --> 01:25:32.129 You can get a very narrow breast and a very underfilled axilla,
01:25:32.140 --> 01:25:34.830 which is not aesthetically pleasing.
01:25:35.299 --> 01:25:39.450 The other aspect is you're pushing the abdomen quite hard to get the width of the flap,
01:25:39.779 --> 01:25:46.379 and so, uh, recognising that a modified radical mastectomy specimen is shaped like an offset
01:25:46.379 --> 01:25:52.250 implant, um, I always try and orientate my flaps obliquely that way you don't have to push
01:25:52.250 --> 01:25:53.729 the abdomen so hard.
01:25:54.220 --> 01:25:57.899 And then it also allows that upper pole to be filled by that fat extension.
01:25:58.759 --> 01:26:03.479 The lower corner then gets folded under that creates the tosis that you need rather than
01:26:03.479 --> 01:26:06.669 folding the whole of the underside of the flap into position.
01:26:07.200 --> 01:26:10.950 As you can see here, here's an example, very narrow breast width.
01:26:11.080 --> 01:26:14.229 You can really see where the axilla is contracted down,
01:26:14.279 --> 01:26:18.600 and we're really concentrating on building out that breast width by reorientating the flap.
01:26:19.209 --> 01:26:22.270 Again, another case, this was a case I inherited, uh,
01:26:22.370 --> 01:26:25.770 with, um, a loss of an expander and again, just filling out that,
01:26:25.830 --> 01:26:28.959 that breast with this patient also had lymphedema that we treated.
01:26:29.370 --> 01:26:33.660 Um, and again, this is the patient before her revisions, but uh just demonstrating that the
01:26:33.660 --> 01:26:34.859 width that we can achieve.
01:26:35.689 --> 01:26:37.890 And so the question is, well, which way do we go?
01:26:37.939 --> 01:26:44.459 And so um this is determined primarily by the perforator locations um but
01:26:44.459 --> 01:26:48.569 also I, I do find it is important to scrutinise the abdominal imaging.
01:26:49.180 --> 01:26:55.180 Most patients will have even thickness between the peramboli or fat and that lower down um by
01:26:55.180 --> 01:26:57.529 the groyne, by by the the the fold.
01:26:58.129 --> 01:26:59.600 But some patients won't.
01:26:59.879 --> 01:27:04.919 They're much fuller on the perambolial region. If you insert those flaps upright,
01:27:05.040 --> 01:27:08.069 they get a fullness in the central part of the breast that I find is,
01:27:08.240 --> 01:27:13.870 is not attractive and is very hard to um to address.
01:27:14.140 --> 01:27:18.439 And so if you turn those flaps, then you can really take advantage of the contours of the
01:27:18.439 --> 01:27:24.350 abdomen. Um, if you look at the template shape of a bra,
01:27:24.589 --> 01:27:30.109 you see that it is, um, uh, it's a cone, and you can learn a lot about how to cone a breast
01:27:30.109 --> 01:27:36.660 reconstruction. Um, and so, um, I find that many of my patients,
01:27:36.819 --> 01:27:42.759 you know, with, with, uh, you know, minitonic breasts, can be very nicely shaped with,
01:27:42.839 --> 01:27:44.370 with a cone reconstruction.
01:27:44.580 --> 01:27:49.279 I also like to link the pedicles. This solves a lot of the geometric issues of
01:27:49.279 --> 01:27:50.580 reaching the internal mammary.
01:27:51.490 --> 01:27:55.080 Um, and I, I quite aggressively comb these flaps, and for instance,
01:27:55.089 --> 01:27:59.129 in this example, high mastectomy scar, to breast on the other side,
01:27:59.290 --> 01:28:02.399 young patient, bipedicled flap, and you know, you can,
01:28:02.450 --> 01:28:07.450 you can cone this flap and, and you can get a, a very nice uh cosmetic outcome that better
01:28:07.450 --> 01:28:10.020 matches what she's trying to achieve on on the other side.
01:28:10.959 --> 01:28:15.259 Again, another patient really likes her native breast, doesn't obviously want anything done to
01:28:15.259 --> 01:28:18.419 that, so you can con the flap, you can get it to look very attractive,
01:28:18.540 --> 01:28:21.410 match the other side, and, and she is refusing to allow me to do,
01:28:21.490 --> 01:28:24.819 do revisions on this flap, but I think it can be slightly improved.
01:28:25.520 --> 01:28:30.040 He coning the other way. So this time the conning is inferiorly and
01:28:30.040 --> 01:28:33.600 again you just have to see how the abdomen's going to fold to decide which way it's going to
01:28:33.600 --> 01:28:36.399 cone. And you know you can argue that the scar on the
01:28:36.399 --> 01:28:41.459 top is not so cosmetically pleasing, but actually sometimes it allows you to cone that
01:28:41.459 --> 01:28:45.069 flap much more effectively and get a much nicer looking breast.
01:28:45.540 --> 01:28:48.390 And then this is just a very small technique that's been around forever,
01:28:48.520 --> 01:28:51.839 but I just want to, you know, just, just reinforce it for those of you who aren't aware
01:28:51.839 --> 01:28:54.850 of it. There's a lot of skin shortage in the upper
01:28:54.850 --> 01:28:59.770 part, the upper mastectomy skin flap, and if you do a lateral back cut,
01:28:59.850 --> 01:29:05.509 you can really release that, um, and, uh, that very much helps in the long term to avoid that
01:29:05.520 --> 01:29:09.520 that constriction of the upper pole. So it's a useful,
01:29:09.850 --> 01:29:12.279 um, old fashioned technique that works very nicely.
01:29:12.490 --> 01:29:13.490 Thank you.
01:29:22.879 --> 01:29:26.759 Those are all like amazing talks. I have so many questions,
01:29:27.240 --> 01:29:31.589 but I wanna know from the audience if anybody has any questions before we start.
01:29:36.629 --> 01:29:40.020 No I think, well, my first question is for you.
01:29:40.370 --> 01:29:43.060 Um, amazing results with this gap.
01:29:43.350 --> 01:29:45.700 My question is about the donor site.
01:29:46.229 --> 01:29:51.629 Um, any like trips, uh, any.
01:29:52.509 --> 01:29:57.560 Ideas of how to make it more cosmetic, especially for unilateral cases.
01:29:57.910 --> 01:29:58.910 Those can be.
01:29:59.959 --> 01:30:01.870 Can be difficult to correct.
01:30:03.089 --> 01:30:09.129 2 Sorry, I, yeah, no, um, I think there's not a huge amount you can do.
01:30:09.520 --> 01:30:12.310 And as I said, I think it's a trade-off on how much chaffroin you do,
01:30:12.319 --> 01:30:15.109 the more chaffin you do, the more of a dip you will get,
01:30:15.189 --> 01:30:16.359 and I, I think it's.
01:30:17.370 --> 01:30:20.089 It's more, it's more about choosing the patient to do it on there,
01:30:20.290 --> 01:30:22.370 um, you know, I think my doing the sides.
01:30:23.950 --> 01:30:25.779 Probably worse, just because I'm trying to get the height,
01:30:25.970 --> 01:30:29.080 um, but I, I, there's not much you can do, you can't, you know,
01:30:29.089 --> 01:30:32.399 because it, it becomes thin and then it goes down and it's already a little bit tight anyway.
01:30:32.859 --> 01:30:34.759 That's, that's one, you know, one of the downsides.
01:30:35.129 --> 01:30:37.959 We do quite a lot of bilaterals and the patients tolerate those much better.
01:30:38.740 --> 01:30:42.339 Um, but I, but I think now with fat transfer and scar release,
01:30:42.790 --> 01:30:45.259 it's it's much easier to get a nicer result in the end,
01:30:45.270 --> 01:30:46.990 with not too much downtime for the patient.
01:30:51.779 --> 01:30:58.049 Yeah, both of you just show very good results with, I think they are all alternative labs as
01:30:58.049 --> 01:31:04.529 you pointed out of uh DF labs because I really think that it is very important that on our
01:31:04.529 --> 01:31:06.799 side if a mastectomy patient.
01:31:07.240 --> 01:31:12.419 Has to be worried not only about the breast that is being reconstructed but also about the
01:31:12.419 --> 01:31:17.279 donor side who have not improved her quality of life, especially in Spain where everybody is
01:31:17.279 --> 01:31:22.430 going to the beach and to the swimming pool and uh it's really a very key point for the woman.
01:31:22.859 --> 01:31:24.549 So could you just say.
01:31:25.109 --> 01:31:30.680 How you indicate and what are the real indications for every one of these flaps
01:31:31.100 --> 01:31:37.089 because I, I really don't believe this is my second choice that the patient is who decides
01:31:37.089 --> 01:31:41.279 what is the second choice depending on the donor site and the tissue available.
01:31:42.009 --> 01:31:48.580 So could you just say what is the? Obviously, it is the patient's choice,
01:31:48.589 --> 01:31:51.180 but it also depends on the constitution of the patient.
01:31:51.470 --> 01:31:57.669 And if you talk about buttock flaps, I think we used to do a lot of first flaps and now we
01:31:57.669 --> 01:32:00.669 reduced it a little bit because I think that.
01:32:01.540 --> 01:32:05.520 This lumbar flap has a nicer consistency, it's easier.
01:32:05.850 --> 01:32:09.240 It's technically a little bit more demanding, but it's easier.
01:32:09.410 --> 01:32:14.370 I restrict my SAP flaps now to patients which really have a sagging buttock,
01:32:14.379 --> 01:32:18.740 the patients who would benefit from having a buttock lift.
01:32:19.009 --> 01:32:21.720 I think these are the ideal candidates for an ASAP flap.
01:32:21.930 --> 01:32:26.040 The ideal candidates for a lumbar flap are obviously bilateral patients,
01:32:26.250 --> 01:32:30.450 for example, the BRCA patients, young patients who don't want prosthetic reconstruction.
01:32:30.779 --> 01:32:34.229 And, and, and most of them don't have a heavy abdomen, uh,
01:32:34.330 --> 01:32:38.109 and, and I think these are, are good candidates. The only thing you have to tell them,
01:32:38.560 --> 01:32:42.120 because there's, there's always a fight when, when we did the ASAP flaps,
01:32:42.160 --> 01:32:44.589 we wanted to have our scar as high as possible.
01:32:44.879 --> 01:32:48.200 But there is the celiac crest, which is the, which is the division in between,
01:32:48.209 --> 01:32:51.080 which limited. So if we have a lumbar flap, we want to scar as
01:32:51.080 --> 01:32:53.720 low as possible. But there is always the illiac crest.
01:32:53.759 --> 01:32:55.160 So with the, with the ASAP flap.
01:32:55.439 --> 01:32:58.410 The disadvantage is if it's not really a sagging buttock,
01:32:58.450 --> 01:33:03.560 you will gonna get a depression, you're gonna get a contoured deficit,
01:33:05.169 --> 01:33:07.879 and you have this less with a with a lumbar flap.
01:33:08.049 --> 01:33:12.080 If the patient has a sagging buttock, I think it's an ideal indication if she doesn't.
01:33:12.930 --> 01:33:16.540 Disagree with that. I think she's a very good candidate for a flap.
01:33:17.089 --> 01:33:21.370 I think the quality of the tissue of the tissue is very important.
01:33:21.830 --> 01:33:28.169 The gluteal tissue is very tight gluteal flap, because if the gluteal tissue is very tight,
01:33:28.250 --> 01:33:33.240 you will have this shelving of your gaps, and this is very difficult to correct.
01:33:33.290 --> 01:33:35.509 You can correct it with liposuction and lipo.
01:33:35.729 --> 01:33:37.330 It's not that easy to correct.
01:33:37.700 --> 01:33:42.259 And, and, and the lumber flap has the advantage that it doesn't have that much uh shelving
01:33:42.259 --> 01:33:45.660 because on top, the lumber flap tends to be thinner, and on the buttock,
01:33:45.700 --> 01:33:47.410 you can harvest as much fat as you want.
01:33:47.750 --> 01:33:51.200 And, and also, uh, in contrary to the D flap was what I said,
01:33:51.209 --> 01:33:54.129 in the D flap, you're always struggling to give the patient enough projection.
01:33:54.169 --> 01:33:57.740 You have to cone the flap, you have to put another flap on the knees.
01:33:58.009 --> 01:34:01.680 We don't believe in stacked flaps. I'm, I, I, I never did a stack flap,
01:34:02.089 --> 01:34:06.649 uh, but you, you, you, you want to have projection, and with these lumbar flaps and
01:34:06.649 --> 01:34:10.810 also with the, with the gluteal flaps, you have a kind of natural projection.
01:34:13.700 --> 01:34:17.000 When we see see the patient, you try and give the patient a choice and just go through all
01:34:17.000 --> 01:34:20.839 the options, but I'd say I recommend, you know, ABC I think you can have,
01:34:20.879 --> 01:34:23.540 and then it's some patients don't want their bottom touched,
01:34:23.660 --> 01:34:25.729 um, others don't want to have them touched, you know, it's,
01:34:25.810 --> 01:34:27.569 it's a patient choice thing.
01:34:27.879 --> 01:34:30.120 I think we've started doing lap flaps as well more and you know,
01:34:30.160 --> 01:34:32.569 I think the tissue generally is softer for a lap flap.
01:34:33.080 --> 01:34:36.560 Um, we probably, I, I do less Scabs than I did used to do because of that.
01:34:40.129 --> 01:34:45.209 There's one other factor in patient choice and surgeon choice because you can't be good at all
01:34:45.209 --> 01:34:49.850 flaps. There are many flaps and you get a favourite
01:34:49.850 --> 01:34:54.129 flap which works for you and you start refining it and you get better and better results.
01:34:54.160 --> 01:34:58.049 So it certainly is not a la carte where you can say you can choose,
01:34:58.129 --> 01:35:00.089 I can do all flaps. I can't do all flaps.
01:35:00.129 --> 01:35:05.200 I can't do a flap as good as it is going to be a factor as well,
01:35:05.250 --> 01:35:06.709 what you can do very well.
01:35:09.529 --> 01:35:14.029 I have a question for you because my second flap of choice is a pad flap.
01:35:14.200 --> 01:35:18.350 I, I love the thigh flaps because, you know, it's a hidden scars,
01:35:18.720 --> 01:35:20.319 um, it's easy dissection.
01:35:21.189 --> 01:35:27.290 But My PA hates them because she's sewing upside down every single time,
01:35:27.859 --> 01:35:32.299 so I began doing them on frog leg. Now I moved to a liotomy position just because
01:35:32.299 --> 01:35:38.410 it's easier closure. Do you have any tips on how to make that flap.
01:35:38.419 --> 01:35:40.049 That's why I do more flaps.
01:35:41.259 --> 01:35:44.189 So I don't like that, not that I don't like path flaps,
01:35:44.259 --> 01:35:47.189 but yes, it's kind of opportunistic.
01:35:47.479 --> 01:35:49.379 Sometimes you come across a big perforator.
01:35:50.240 --> 01:35:56.830 I when I lift a tug, I start doing a tug and I come from the back and I see a
01:35:56.830 --> 01:35:59.509 perforator. I suddenly sort of make it a path flap.
01:35:59.549 --> 01:36:00.779 That's about the only time.
01:36:01.149 --> 01:36:06.410 But then I do it supine with a leg open, but it's a bit of a strain on your neck.
01:36:07.629 --> 01:36:12.350 Yeah, it's not very pleasant. So that's why I go on to tug flaps and it's
01:36:12.350 --> 01:36:17.310 expedient in the sense the breast surgeon is working and you've got the flap out before the
01:36:17.310 --> 01:36:20.520 mastectomy, so. I think that the indication in,
01:36:20.580 --> 01:36:25.140 in, in, in my practise, the indication for the inner tie flaps is less because I think it has
01:36:25.140 --> 01:36:28.459 to do with the with the size of the patients obviously and I think that the American
01:36:28.459 --> 01:36:33.819 patients might be a little bit bigger and, and, and most of the time that you can't do a deep
01:36:33.819 --> 01:36:40.450 flap it means that most of the time you have to, we have 10 patients and then the thys don't
01:36:40.450 --> 01:36:41.850 work out that good for me.
01:36:42.509 --> 01:36:45.020 I think for us with the, with the pap flap, we have lithotomy,
01:36:45.069 --> 01:36:46.779 so the Pfizer up there.
01:36:47.109 --> 01:36:49.870 So the closures is not not as difficult, I think.
01:36:50.899 --> 01:36:53.589 Yeah, I think it was yesterday.
01:36:54.089 --> 01:36:59.049 Uh, somebody talked about the quality of life with a side thought was construction was the
01:36:59.049 --> 01:37:02.490 worst. I, I think somebody said that in one of the
01:37:02.490 --> 01:37:07.720 publications that that no didn't, OK, yeah.
01:37:10.379 --> 01:37:11.700 But I, I agree with.
01:37:11.939 --> 01:37:15.799 I think that the, the legs normally are there is no,
01:37:16.299 --> 01:37:21.540 at least in Europe, a lot of hanging tissue compared to abdomen that is like a natural
01:37:21.540 --> 01:37:22.609 hanging area.
01:37:22.979 --> 01:37:29.500 So I really don't just think that the sizes are a good donor site if you can offer uh a side
01:37:29.500 --> 01:37:32.020 lift. That is the real indication.
01:37:32.060 --> 01:37:36.259 It's like when we can offer a real abdominoplasty in the lab that's the real
01:37:36.259 --> 01:37:40.560 benefit. And otherwise it's true that sometimes patient
01:37:40.850 --> 01:37:41.950 is not for autologous.
01:37:42.330 --> 01:37:48.759 We try to push, uh, the autologous indication. Maybe we have to combine fat grafting,
01:37:48.770 --> 01:37:54.490 uh, other techniques that we have in our armamentarium and not just always try to look
01:37:54.490 --> 01:37:59.720 after the toor side because the sequela is there although we preserve the muscle although
01:37:59.729 --> 01:38:03.850 although we preserve the, the, the nerves there is a site.
01:38:07.709 --> 01:38:14.089 Uh, Ben had apparently with the vertical orientation of the skin island both fort and
01:38:14.089 --> 01:38:19.140 for pop flap, the complication rate is lower considering, uh,
01:38:19.149 --> 01:38:25.549 lymphoa, you know, sensation problems and the, the, the scar problems that you already
01:38:25.549 --> 01:38:29.520 described. You still prefer the orientation, uh,
01:38:29.529 --> 01:38:33.120 in a horizontal uh shape versus vertical.
01:38:33.609 --> 01:38:36.700 For the tug, yes, for a pap, it's much more oblique.
01:38:37.049 --> 01:38:40.319 It'll be the anterior part will go to the labial commiser,
01:38:40.890 --> 01:38:44.359 and at the back, it will go up to the gluteal crease.
01:38:44.609 --> 01:38:47.689 So it will be much more oblique for a tug, it's much.
01:38:49.129 --> 01:38:50.220 I still like you sir.
01:38:53.080 --> 01:39:00.000 On the note of this lumber flaps, with regards to the 3 changes of pushing or
01:39:00.040 --> 01:39:03.839 two changes of pushing, why would you do that if you harvest the flap first,
01:39:03.879 --> 01:39:05.080 that's how we do it.
01:39:05.439 --> 01:39:06.970 Is it the ischemia time.
01:39:07.700 --> 01:39:08.919 You're concerned about.
01:39:10.220 --> 01:39:13.770 Yeah, a little bit, yes. The, the, the thing is that we need this
01:39:13.770 --> 01:39:16.649 interposition graph. We want this interposition graft.
01:39:16.689 --> 01:39:20.450 I think it's key in the lumbar flap, and we do it also for gap flaps.
01:39:20.490 --> 01:39:23.569 So you want to see your vessels, you do the mastectomy thing and then you take the
01:39:23.569 --> 01:39:26.250 interposition graph. And I think it's better to let the
01:39:26.250 --> 01:39:30.919 interposition graft rest a little bit and letting your flap rest over there.
01:39:31.250 --> 01:39:32.439 Gets you a little bit more.
01:39:32.970 --> 01:39:38.000 Nervous, I think, and, and for us this this changing of position is not such a big point,
01:39:38.770 --> 01:39:43.049 but we didn't address that. What is the one of the main problems with SAPs
01:39:43.049 --> 01:39:47.529 and lumbar flaps obviously is seroma, and you have to really take care of that.
01:39:47.629 --> 01:39:52.620 So we do a kind of a vest over pan closure we use stacking sutures and also whenever I have a
01:39:52.620 --> 01:39:57.770 seroma, the first thing I do, I drain it and I inject corticosteroids because I think that it
01:39:57.770 --> 01:40:00.970 is really an inflammatory disease and it also reduces the pain.
01:40:01.500 --> 01:40:06.140 Sometimes you have to be very careful with your uh lumbar and your S gap flaps because it's
01:40:06.140 --> 01:40:09.779 like in a, in, in a deep flap, the patients tend to bend over because they,
01:40:09.859 --> 01:40:12.140 they feel that, and if they do it in the back, you know,
01:40:12.299 --> 01:40:15.259 they, they, they, they, they start walking a little bit crippled and then.
01:40:15.990 --> 01:40:20.770 Sometimes in the beginning and we really needed physiotherapy to get this out again so you have
01:40:20.770 --> 01:40:27.600 to take really care of doing the closure and this closure takes them about the same
01:40:27.600 --> 01:40:32.720 time as me doing this interposition graft so there is not much time lost by changing
01:40:32.720 --> 01:40:36.009 position. It's Wonderful.
01:40:36.220 --> 01:40:39.310 So I think the interest of time we're gonna end this session,
01:40:39.700 --> 01:40:43.649 but if anybody has other questions we can talk during lunch.
Microsurgical Reconstruction
10 July 2024
This session from the London Breast Meeting 2024 includes several presentations on microsurgical reconstruction.
This session from the London Breast Meeting 2024 covers microsurgical reconstruction. The session is chaired by Venkat Ramakrishnan & Koen Van Landuyt. The presentations in this video are:
- Nipple sparing Mastectomy and Free Flaps Reconstruction, Ed Chang
- Aesthetic considerations- patient vs surgeon outcomes, Andrea Moreira
- Fat necrosis in flaps - strategies to avoid this and the role of imaging, Gemma Pons
- Discussion
- Tips and Tricks of Autologous Reconstruction
- The SGAP flap, Paul Roblin
- The LAP flap, Koen Van Landuyt
- Thigh flaps, Venkat Ramakrishnan
- Insetting of the delayed flap reconstruction, Mark Schaverien
International, CPD certified conference that assembles some of the world’s most highly respected professionals working in the field of aesthetic and reconstructive breast surgery today.